A randomized controlled trial of pectoralis major myofascial release massage for breastfeeding mothers: breast pain, engorgement, and newborns' breast milk intake and sleeping patterns.
Won-Ryung Choi, Myung-Haeng Hur, Yeon-Suk Kim, Ju-Ri Kim
{"title":"A randomized controlled trial of pectoralis major myofascial release massage for breastfeeding mothers: breast pain, engorgement, and newborns' breast milk intake and sleeping patterns.","authors":"Won-Ryung Choi, Myung-Haeng Hur, Yeon-Suk Kim, Ju-Ri Kim","doi":"10.4069/kjwhn.2023.03.15","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Supportive interventions to improve breastfeeding practice are needed in nursing. This study investigated the effects of pectoralis major myofascial release massage (MRM) on breast pain and engorgement among breastfeeding mothers and on breast milk intake and sleep patterns among newborns.</p><p><strong>Methods: </strong>Breastfeeding mothers who had delivered between 37 and 43 weeks and had 7-to 14-dayold newborns were recruited from a postpartum care center in Gunpo, Korea. Participants were randomized to the MRM or control group. The outcome variables were breast pain and breast engorgement among breastfeeding mothers and breast milk intake and sleep time among newborns. The experimental treatment involved applying MRM to separate the pectoralis major muscle and the underlying breast tissue in the chest. After delivery, the first MRM session (MRM I) was provided by a breast specialist nurse, and the second (MRM II) was administered 48 hours after MRM I.</p><p><strong>Results: </strong>Following MRM, breast pain (MRM I: t=-5.38, p<.001; MRM II: t=-10.05, p<.001), breast engorgement (MRM I: right, t=-1.68, p =.100; left, t=-2.13, p=.037 and MRM II: right, t=-4.50, p<.001; left, t=-3.74, p<.001), and newborn breast milk intake (MRM I: t=3.10, p=.003; MRM II: t=3.09, p=.003) differed significantly between the groups.</p><p><strong>Conclusion: </strong>MRM effectively reduced breast engorgement and breast pain in breastfeeding mothers, reducing the need for formula supplementation, and increasing newborns' breast milk intake. Therefore, MRM can be utilized as an effective nursing intervention to alleviate discomfort during breastfeeding and to improve the rate of breastfeeding practice (clinical trial number: KCT0002436).</p>","PeriodicalId":30467,"journal":{"name":"Korean Journal of Women Health Nursing","volume":"29 1","pages":"66-75"},"PeriodicalIF":1.2000,"publicationDate":"2023-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10085664/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Women Health Nursing","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4069/kjwhn.2023.03.15","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/3/31 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"NURSING","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Supportive interventions to improve breastfeeding practice are needed in nursing. This study investigated the effects of pectoralis major myofascial release massage (MRM) on breast pain and engorgement among breastfeeding mothers and on breast milk intake and sleep patterns among newborns.
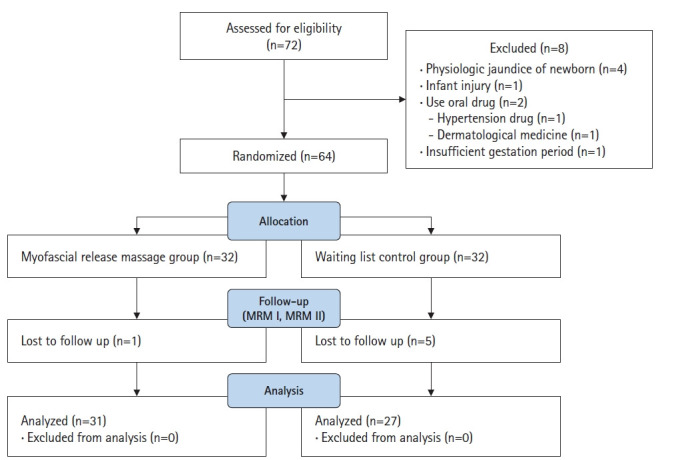
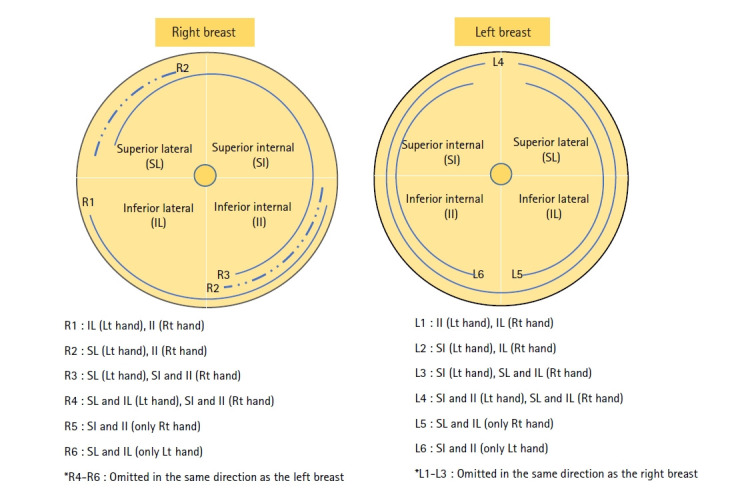
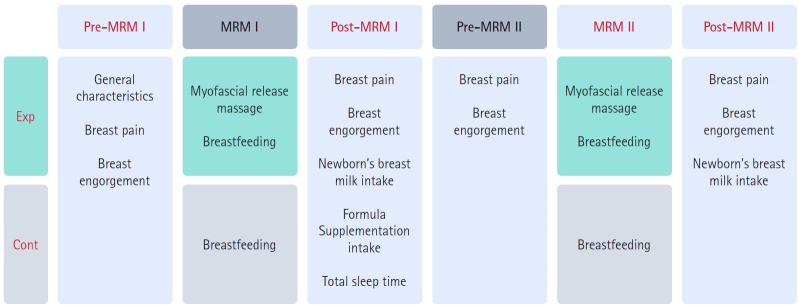
Methods: Breastfeeding mothers who had delivered between 37 and 43 weeks and had 7-to 14-dayold newborns were recruited from a postpartum care center in Gunpo, Korea. Participants were randomized to the MRM or control group. The outcome variables were breast pain and breast engorgement among breastfeeding mothers and breast milk intake and sleep time among newborns. The experimental treatment involved applying MRM to separate the pectoralis major muscle and the underlying breast tissue in the chest. After delivery, the first MRM session (MRM I) was provided by a breast specialist nurse, and the second (MRM II) was administered 48 hours after MRM I.
Results: Following MRM, breast pain (MRM I: t=-5.38, p<.001; MRM II: t=-10.05, p<.001), breast engorgement (MRM I: right, t=-1.68, p =.100; left, t=-2.13, p=.037 and MRM II: right, t=-4.50, p<.001; left, t=-3.74, p<.001), and newborn breast milk intake (MRM I: t=3.10, p=.003; MRM II: t=3.09, p=.003) differed significantly between the groups.
Conclusion: MRM effectively reduced breast engorgement and breast pain in breastfeeding mothers, reducing the need for formula supplementation, and increasing newborns' breast milk intake. Therefore, MRM can be utilized as an effective nursing intervention to alleviate discomfort during breastfeeding and to improve the rate of breastfeeding practice (clinical trial number: KCT0002436).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


