Alessandra Mangone, Barbara Altieri, Mario Detomas, Alessandro Prete, Haider Abbas, Miriam Asia, Yasir S Elhassan, Giovanna Mantovani, Cristina L Ronchi
{"title":"Inflammation-based scores as predictors of treatment response in advanced adrenocortical carcinoma.","authors":"Alessandra Mangone, Barbara Altieri, Mario Detomas, Alessandro Prete, Haider Abbas, Miriam Asia, Yasir S Elhassan, Giovanna Mantovani, Cristina L Ronchi","doi":"10.1530/ERC-22-0372","DOIUrl":null,"url":null,"abstract":"<p><p>Treatment for advanced adrenocortical carcinoma (ACC) consists of mitotane alone or combined with etoposide, doxorubicin, and cisplatin (EDP). Although both therapies are widely used, markers of response are still lacking. Since inflammation-based scores have been proposed as prognostic factors in ACC, we aimed to investigate their role in predicting the response to first-line chemotherapy. We performed a retrospective analysis of patients with advanced ACC treated with mitotane monotherapy or EDP ± mitotane. Clinical parameters (tumour stage at diagnosis, resection status, Ki67, time from diagnosis to treatment start, performance status, plasma mitotane levels, time in mitotane target ≥ 80%, clinically overt cortisol hypersecretion), and pretreatment inflammation-based scores (neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), monocyte-to-lymphocyte ratio, derived neutrophil-to-lymphocyte ratio) were investigated. The primary endpoints were overall survival (OS) and time-to-progression (TTP) from treatment initiation, the secondary endpoint was the best objective response to treatment. We included 90 patients (59% = women, median age = 51 years) treated with mitotane monotherapy (n = 40) or EDP ± mitotane (n = 50). In the mitotane monotherapy cohort, NLR ≥ 5 and PLR ≥ 190 predicted shorter OS (hazard ratio (HR): 145.83, 95% CI: 1.87-11,323.83; HR: 165.50, 95% CI: 1.76-15,538.04, respectively), remaining significant at multivariable analysis including clinical variables. NLR was also associated with shorter TTP (HR: 2.58, 95% CI: 1.28-5.20), but only at univariable analysis. Patients with NLR ≥ 5 showed a worse treatment response than those with NLR < 5 (P = 0.040). In the EDP ± mitotane cohort, NLR ≥ 5 predicted shorter OS (HR: 2.52, 95% CI: 1.30-4.88) and TTP (HR: 1.95, 95% CI: 1.04-3.66) at univariable analysis. In conclusion, inflammation-based scores, calculated from routinely measured parameters, may help predict response to chemotherapy in advanced ACC.</p>","PeriodicalId":11654,"journal":{"name":"Endocrine-related cancer","volume":"30 4","pages":""},"PeriodicalIF":4.6000,"publicationDate":"2023-03-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10083578/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrine-related cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1530/ERC-22-0372","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/4/1 0:00:00","PubModel":"Print","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
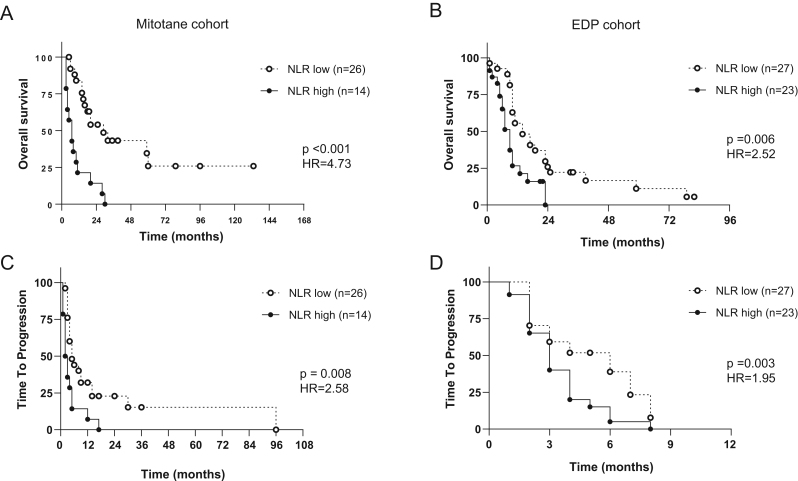
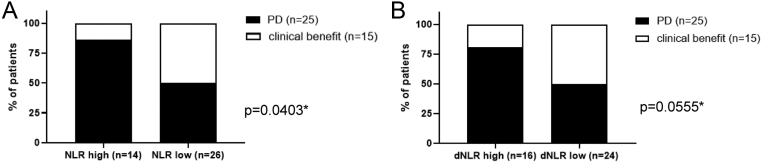
Treatment for advanced adrenocortical carcinoma (ACC) consists of mitotane alone or combined with etoposide, doxorubicin, and cisplatin (EDP). Although both therapies are widely used, markers of response are still lacking. Since inflammation-based scores have been proposed as prognostic factors in ACC, we aimed to investigate their role in predicting the response to first-line chemotherapy. We performed a retrospective analysis of patients with advanced ACC treated with mitotane monotherapy or EDP ± mitotane. Clinical parameters (tumour stage at diagnosis, resection status, Ki67, time from diagnosis to treatment start, performance status, plasma mitotane levels, time in mitotane target ≥ 80%, clinically overt cortisol hypersecretion), and pretreatment inflammation-based scores (neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), monocyte-to-lymphocyte ratio, derived neutrophil-to-lymphocyte ratio) were investigated. The primary endpoints were overall survival (OS) and time-to-progression (TTP) from treatment initiation, the secondary endpoint was the best objective response to treatment. We included 90 patients (59% = women, median age = 51 years) treated with mitotane monotherapy (n = 40) or EDP ± mitotane (n = 50). In the mitotane monotherapy cohort, NLR ≥ 5 and PLR ≥ 190 predicted shorter OS (hazard ratio (HR): 145.83, 95% CI: 1.87-11,323.83; HR: 165.50, 95% CI: 1.76-15,538.04, respectively), remaining significant at multivariable analysis including clinical variables. NLR was also associated with shorter TTP (HR: 2.58, 95% CI: 1.28-5.20), but only at univariable analysis. Patients with NLR ≥ 5 showed a worse treatment response than those with NLR < 5 (P = 0.040). In the EDP ± mitotane cohort, NLR ≥ 5 predicted shorter OS (HR: 2.52, 95% CI: 1.30-4.88) and TTP (HR: 1.95, 95% CI: 1.04-3.66) at univariable analysis. In conclusion, inflammation-based scores, calculated from routinely measured parameters, may help predict response to chemotherapy in advanced ACC.
期刊介绍:
Endocrine-Related Cancer is an official flagship journal of the Society for Endocrinology and is endorsed by the European Society of Endocrinology, the United Kingdom and Ireland Neuroendocrine Society, and the Japanese Hormones and Cancer Society.
Endocrine-Related Cancer provides a unique international forum for the publication of high quality original articles describing novel, cutting edge basic laboratory, translational and clinical investigations of human health and disease focusing on endocrine neoplasias and hormone-dependent cancers; and for the publication of authoritative review articles in these topics.
Endocrine neoplasias include adrenal cortex, breast, multiple endocrine neoplasia, neuroendocrine tumours, ovary, prostate, paraganglioma, parathyroid, pheochromocytoma pituitary, testes, thyroid and hormone-dependent cancers. Neoplasias affecting metabolism and energy production such as bladder, bone, kidney, lung, and head and neck, are also considered.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


