Insook Cho, MiSoon Kim, Mi Ra Song, Patricia C Dykes
{"title":"Evaluation of an approach to clinical decision support for preventing inpatient falls: a pragmatic trial.","authors":"Insook Cho, MiSoon Kim, Mi Ra Song, Patricia C Dykes","doi":"10.1093/jamiaopen/ooad019","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To assess whether a fall-prevention clinical decision support (CDS) approach using electronic analytics that stimulates risk-targeted interventions is associated with reduced rates of falls and injurious falls.</p><p><strong>Materials and methods: </strong>The CDS intervention included a machine-learning prediction algorithm, individual risk-factor identification, and guideline-based prevention recommendations. After a 5-month plan-do-study-act quality improvement initiative, the CDS intervention was implemented at an academic tertiary hospital and compared with the usual care using a pretest (lasting 24 months and involving 23 498 patients) and posttest (lasting 13 months and involving 17 341 patients) design in six nursing units. Primary and secondary outcomes were the rates of falls and injurious falls per 1000 hospital days, respectively. Outcome measurements were tested using a priori Poisson regression and adjusted with patient-level covariates. Subgroup analyses were conducted according to age.</p><p><strong>Results: </strong>The age distribution, sex, hospital and unit lengths of stay, number of secondary diagnoses, fall history, condition at admission, and overall fall rate per 1000 hospital days did not differ significantly between the intervention and control periods before (1.88 vs 2.05, respectively, <i>P </i>=<i> </i>.1764) or after adjusting for demographics. The injurious-falls rate per 1000 hospital days decreased significantly before (0.68 vs 0.45, <i>P </i>=<i> </i>.0171) and after (rate difference = -0.64, <i>P </i>=<i> </i>.0212) adjusting for demographics. The differences in injury rates were greater among patients aged at least 65 years.</p><p><strong>Conclusions: </strong>This study suggests that a well-designed CDS intervention employing electronic analytics was associated with a decrease in fall-related injuries. The benefits from this intervention were greater in elderly patients aged at least 65 years.</p><p><strong>Trial registration: </strong>This study was conducted as part of a more extensive study registered with the Clinical Research Information Service (CRIS) (KCT0005378).</p>","PeriodicalId":36278,"journal":{"name":"JAMIA Open","volume":null,"pages":null},"PeriodicalIF":2.5000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10079353/pdf/","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMIA Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jamiaopen/ooad019","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 2
Abstract
Objectives: To assess whether a fall-prevention clinical decision support (CDS) approach using electronic analytics that stimulates risk-targeted interventions is associated with reduced rates of falls and injurious falls.
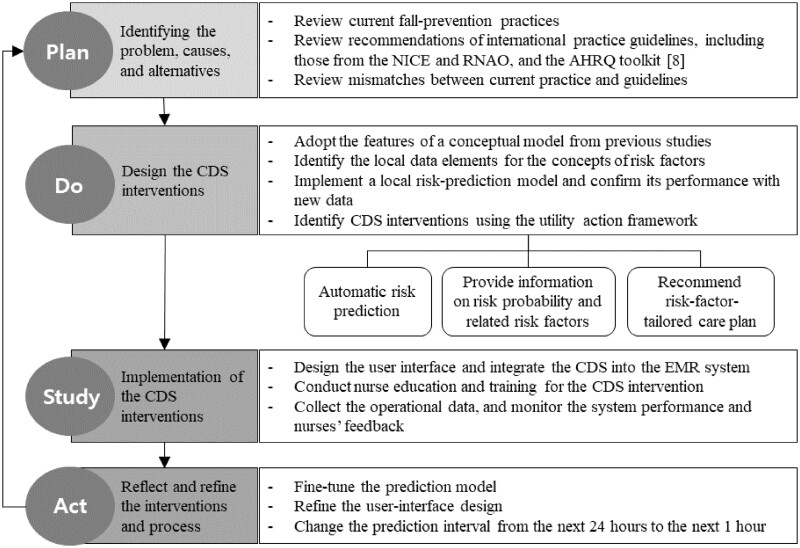
Materials and methods: The CDS intervention included a machine-learning prediction algorithm, individual risk-factor identification, and guideline-based prevention recommendations. After a 5-month plan-do-study-act quality improvement initiative, the CDS intervention was implemented at an academic tertiary hospital and compared with the usual care using a pretest (lasting 24 months and involving 23 498 patients) and posttest (lasting 13 months and involving 17 341 patients) design in six nursing units. Primary and secondary outcomes were the rates of falls and injurious falls per 1000 hospital days, respectively. Outcome measurements were tested using a priori Poisson regression and adjusted with patient-level covariates. Subgroup analyses were conducted according to age.
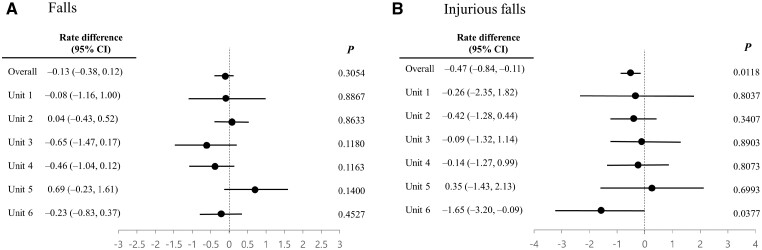
Results: The age distribution, sex, hospital and unit lengths of stay, number of secondary diagnoses, fall history, condition at admission, and overall fall rate per 1000 hospital days did not differ significantly between the intervention and control periods before (1.88 vs 2.05, respectively, P =.1764) or after adjusting for demographics. The injurious-falls rate per 1000 hospital days decreased significantly before (0.68 vs 0.45, P =.0171) and after (rate difference = -0.64, P =.0212) adjusting for demographics. The differences in injury rates were greater among patients aged at least 65 years.
Conclusions: This study suggests that a well-designed CDS intervention employing electronic analytics was associated with a decrease in fall-related injuries. The benefits from this intervention were greater in elderly patients aged at least 65 years.
Trial registration: This study was conducted as part of a more extensive study registered with the Clinical Research Information Service (CRIS) (KCT0005378).
目的:评估使用电子分析刺激风险目标干预的预防跌倒临床决策支持(CDS)方法是否与降低跌倒和伤害性跌倒率相关。材料和方法:CDS干预包括机器学习预测算法、个体风险因素识别和基于指南的预防建议。经过5个月的计划-研究-行动质量改进倡议,在一家三级学术医院实施了CDS干预措施,并在6个护理单位采用前测(持续24个月,涉及23498名患者)和后测(持续13个月,涉及17341名患者)设计与常规护理进行了比较。主要结局和次要结局分别是每1000个住院日的跌倒率和伤害性跌倒率。结果测量使用先验泊松回归进行检验,并用患者水平协变量进行调整。按年龄进行亚组分析。结果:年龄分布、性别、住院天数、二次诊断次数、跌倒史、入院时病情和每1000住院日总跌倒率在干预前和调整人口统计学因素后均无显著差异(分别为1.88 vs 2.05, P = 0.1764)。在人口统计学调整前(0.68 vs 0.45, P = 0.0171)和调整后(率差= -0.64,P = 0.0212),每1000个住院日受伤跌倒率显著下降。在65岁以上的患者中,损伤率的差异更大。结论:本研究表明,采用电子分析的精心设计的CDS干预与跌倒相关损伤的减少有关。这种干预在65岁以上的老年患者中获益更大。试验注册:本研究是临床研究信息服务(CRIS) (KCT0005378)注册的更广泛研究的一部分。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


