Mohammed S Abdalla, Ben Carlton Smith, Allison Kirchner, Maria Abu Nseir, Mousab Mokhtar, Ahmed Abdulrahman, Eltaib Saad
{"title":"Subarachnoid Hemorrhage From Cavernous Malformation Masquerading as Myocardial Infarction.","authors":"Mohammed S Abdalla, Ben Carlton Smith, Allison Kirchner, Maria Abu Nseir, Mousab Mokhtar, Ahmed Abdulrahman, Eltaib Saad","doi":"10.14740/jmc4064","DOIUrl":null,"url":null,"abstract":"<p><p>Intracranial hemorrhage, including subarachnoid hemorrhage (SAH), is associated with many cardiac effects, including cardiac rhythm abnormalities, ischemic electrocardiographic (ECG) changes, elevated cardiac troponin levels, and regional wall motion abnormalities on echocardiogram. About 40% of patients with SAH demonstrate increased serum markers for myocardial necrosis. Approximately 10% of patients with SAH demonstrate left ventricular (LV) wall motion abnormalities; a subset of these patients will have irreversible myocardial damage, but most regain LV function in several weeks. Cardiac effects of SAH are thought to be a result of an imbalance of the autonomic nervous system with resultant increased catecholamine effect on the myocardial cells rather than due to preexisting coronary artery disease. These cardiovascular complications carry a prognostic significance in patients with SAH and can also be misdiagnosed as primary cardiac problems and delay the diagnosis of SAH. Herein, we present a case of a 68-year-old female who presented to the emergency department with acute onset of upper back and neck pain. She was initially misdiagnosed with myocardial infarction in view of the ischemic changes in the ECG and elevated cardiac troponins. She was started on antiplatelets and anticoagulation but was later found to have a negative coronary angiography and was diagnosed with SAH via a computed tomography (CT) scan. Intracranial hemorrhage can be associated with elevated cardiac enzymes and ECG changes and can sometimes masquerade as an acute coronary syndrome (ACS). A careful history and examination and a high index of clinical suspicion are pivotal in such cases since early diagnosis significantly impacts prognosis and prevents the inadvertent use of antiplatelets and anticoagulation, which can be detrimental if used in such cases.</p>","PeriodicalId":16279,"journal":{"name":"Journal of Medical Cases","volume":"14 3","pages":"105-110"},"PeriodicalIF":0.0000,"publicationDate":"2023-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3b/7b/jmc-14-105.PMC10079361.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Medical Cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jmc4064","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
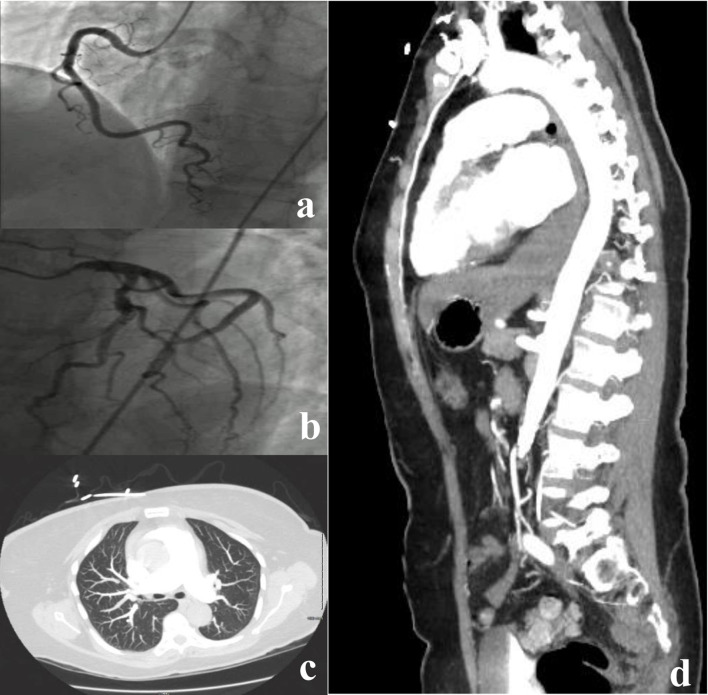
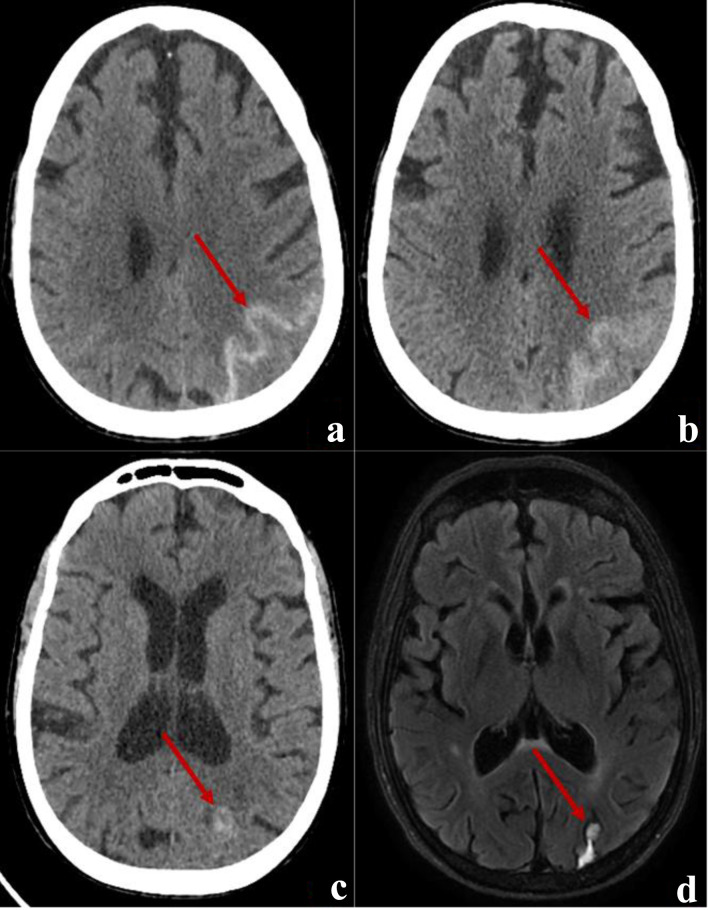
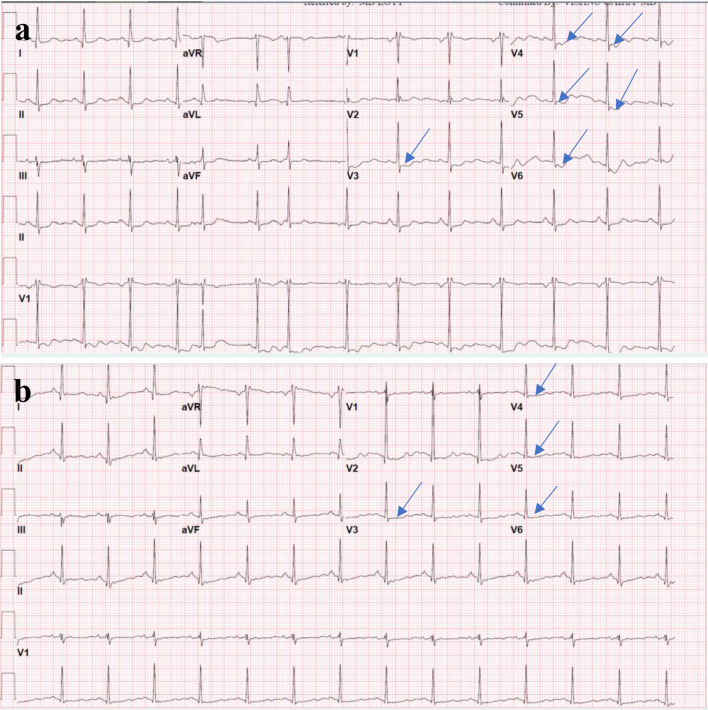
Intracranial hemorrhage, including subarachnoid hemorrhage (SAH), is associated with many cardiac effects, including cardiac rhythm abnormalities, ischemic electrocardiographic (ECG) changes, elevated cardiac troponin levels, and regional wall motion abnormalities on echocardiogram. About 40% of patients with SAH demonstrate increased serum markers for myocardial necrosis. Approximately 10% of patients with SAH demonstrate left ventricular (LV) wall motion abnormalities; a subset of these patients will have irreversible myocardial damage, but most regain LV function in several weeks. Cardiac effects of SAH are thought to be a result of an imbalance of the autonomic nervous system with resultant increased catecholamine effect on the myocardial cells rather than due to preexisting coronary artery disease. These cardiovascular complications carry a prognostic significance in patients with SAH and can also be misdiagnosed as primary cardiac problems and delay the diagnosis of SAH. Herein, we present a case of a 68-year-old female who presented to the emergency department with acute onset of upper back and neck pain. She was initially misdiagnosed with myocardial infarction in view of the ischemic changes in the ECG and elevated cardiac troponins. She was started on antiplatelets and anticoagulation but was later found to have a negative coronary angiography and was diagnosed with SAH via a computed tomography (CT) scan. Intracranial hemorrhage can be associated with elevated cardiac enzymes and ECG changes and can sometimes masquerade as an acute coronary syndrome (ACS). A careful history and examination and a high index of clinical suspicion are pivotal in such cases since early diagnosis significantly impacts prognosis and prevents the inadvertent use of antiplatelets and anticoagulation, which can be detrimental if used in such cases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


