Inequities in Rural and Urban Health Care Utilization Among Individuals Diagnosed With Inflammatory Bowel Disease: A Retrospective Population-Based Cohort Study From Saskatchewan, Canada.
Juan Nicolás Peña-Sánchez, Jessica Amankwah Osei, Noelle Rohatinsky, Xinya Lu, Tracie Risling, Ian Boyd, Kendall Wicks, Mike Wicks, Carol-Lynne Quintin, Alyssa Dickson, Sharyle A Fowler
{"title":"Inequities in Rural and Urban Health Care Utilization Among Individuals Diagnosed With Inflammatory Bowel Disease: A Retrospective Population-Based Cohort Study From Saskatchewan, Canada.","authors":"Juan Nicolás Peña-Sánchez, Jessica Amankwah Osei, Noelle Rohatinsky, Xinya Lu, Tracie Risling, Ian Boyd, Kendall Wicks, Mike Wicks, Carol-Lynne Quintin, Alyssa Dickson, Sharyle A Fowler","doi":"10.1093/jcag/gwac015","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Rural dwellers with inflammatory bowel disease (IBD) face barriers to accessing specialized health services. We aimed to contrast health care utilization between rural and urban residents diagnosed with IBD in Saskatchewan, Canada.</p><p><strong>Methods: </strong>We completed a population-based retrospective study from 1998/1999 to 2017/2018 using administrative health databases. A validated algorithm was used to identify incident IBD cases aged 18+. Rural/urban residence was assigned at IBD diagnosis. Outpatient (gastroenterology visits, lower endoscopies, and IBD medications claims) and inpatient (IBD-specific and IBD-related hospitalizations, and surgeries for IBD) outcomes were measured after IBD diagnosis. Cox proportional hazard, negative binomial, and logistic models were used to evaluate associations adjusting by sex, age, neighbourhood income quintile, and disease type. Hazard ratios (HR), incidence rate ratios (IRR), odds ratios (OR), and 95% confidence intervals (95% CI) were reported.</p><p><strong>Results: </strong>From 5,173 incident IBD cases, 1,544 (29.8%) were living in rural Saskatchewan at IBD diagnosis. Compared to urban dwellers, rural residents had fewer gastroenterology visits (HR = 0.82, 95% CI: 0.77-0.88), were less likely to have a gastroenterologist as primary IBD care provider (OR = 0.60, 95% CI: 0.51-0.70), and had lower endoscopies rates (IRR = 0.92, 95% CI: 0.87-0.98) and more 5-aminosalicylic acid claims (HR = 1.10, 95% CI: 1.02-1.18). Rural residents had a higher risk and rates of IBD-specific (HR = 1.23, 95% CI: 1.13-1.34; IRR = 1.22, 95% CI: 1.09-1.37) and IBD-related (HR = 1.20, 95% CI: 1.11-1.31; IRR = 1.23, 95% CI: 1.10-1.37) hospitalizations than their urban counterparts.</p><p><strong>Conclusion: </strong>We identified rural-urban disparities in IBD health care utilization that reflect rural-urban inequities in the access to IBD care. These inequities require attention to promote health care innovation and equitable management of patients with IBD living in rural areas.</p>","PeriodicalId":17263,"journal":{"name":"Journal of the Canadian Association of Gastroenterology","volume":"6 2","pages":"55-63"},"PeriodicalIF":0.0000,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/73/5b/gwac015.PMC10071297.pdf","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Canadian Association of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jcag/gwac015","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 4
Abstract
Background: Rural dwellers with inflammatory bowel disease (IBD) face barriers to accessing specialized health services. We aimed to contrast health care utilization between rural and urban residents diagnosed with IBD in Saskatchewan, Canada.
Methods: We completed a population-based retrospective study from 1998/1999 to 2017/2018 using administrative health databases. A validated algorithm was used to identify incident IBD cases aged 18+. Rural/urban residence was assigned at IBD diagnosis. Outpatient (gastroenterology visits, lower endoscopies, and IBD medications claims) and inpatient (IBD-specific and IBD-related hospitalizations, and surgeries for IBD) outcomes were measured after IBD diagnosis. Cox proportional hazard, negative binomial, and logistic models were used to evaluate associations adjusting by sex, age, neighbourhood income quintile, and disease type. Hazard ratios (HR), incidence rate ratios (IRR), odds ratios (OR), and 95% confidence intervals (95% CI) were reported.
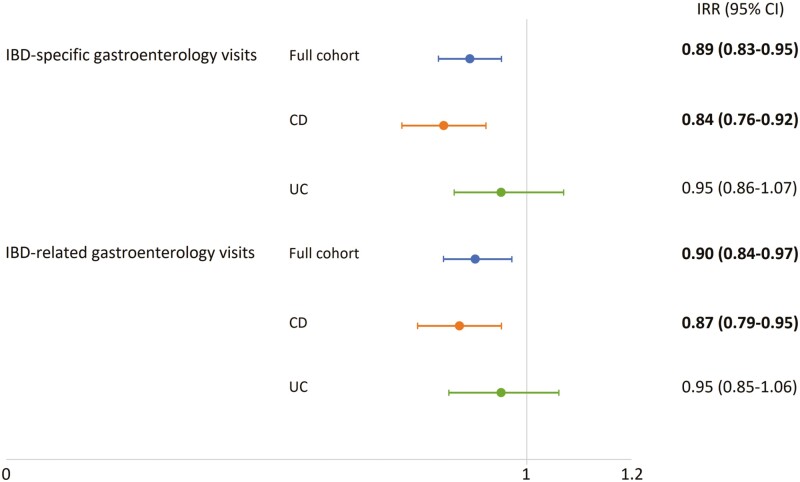
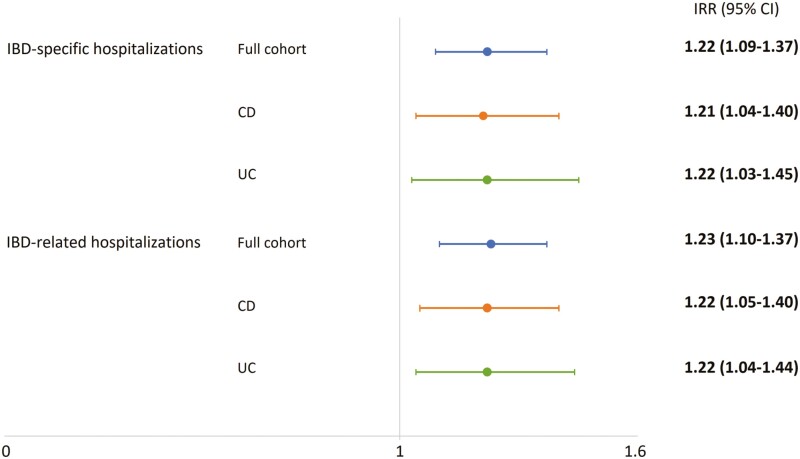
Results: From 5,173 incident IBD cases, 1,544 (29.8%) were living in rural Saskatchewan at IBD diagnosis. Compared to urban dwellers, rural residents had fewer gastroenterology visits (HR = 0.82, 95% CI: 0.77-0.88), were less likely to have a gastroenterologist as primary IBD care provider (OR = 0.60, 95% CI: 0.51-0.70), and had lower endoscopies rates (IRR = 0.92, 95% CI: 0.87-0.98) and more 5-aminosalicylic acid claims (HR = 1.10, 95% CI: 1.02-1.18). Rural residents had a higher risk and rates of IBD-specific (HR = 1.23, 95% CI: 1.13-1.34; IRR = 1.22, 95% CI: 1.09-1.37) and IBD-related (HR = 1.20, 95% CI: 1.11-1.31; IRR = 1.23, 95% CI: 1.10-1.37) hospitalizations than their urban counterparts.
Conclusion: We identified rural-urban disparities in IBD health care utilization that reflect rural-urban inequities in the access to IBD care. These inequities require attention to promote health care innovation and equitable management of patients with IBD living in rural areas.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


