Mechanical power and 30-day mortality in mechanically ventilated, critically ill patients with and without Coronavirus Disease-2019: a hospital registry study.
Basit A Azizi, Ricardo Munoz-Acuna, Aiman Suleiman, Elena Ahrens, Simone Redaelli, Tim M Tartler, Guanqing Chen, Boris Jung, Daniel Talmor, Elias N Baedorf-Kassis, Maximilian S Schaefer
{"title":"Mechanical power and 30-day mortality in mechanically ventilated, critically ill patients with and without Coronavirus Disease-2019: a hospital registry study.","authors":"Basit A Azizi, Ricardo Munoz-Acuna, Aiman Suleiman, Elena Ahrens, Simone Redaelli, Tim M Tartler, Guanqing Chen, Boris Jung, Daniel Talmor, Elias N Baedorf-Kassis, Maximilian S Schaefer","doi":"10.1186/s40560-023-00662-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Previous studies linked a high intensity of ventilation, measured as mechanical power, to mortality in patients suffering from \"classic\" ARDS. By contrast, mechanically ventilated patients with a diagnosis of COVID-19 may present with intact pulmonary mechanics while undergoing mechanical ventilation for longer periods of time. We investigated whether an association between higher mechanical power and mortality is modified by a diagnosis of COVID-19.</p><p><strong>Methods: </strong>This retrospective study included critically ill, adult patients who were mechanically ventilated for at least 24 h between March 2020 and December 2021 at a tertiary healthcare facility in Boston, Massachusetts. The primary exposure was median mechanical power during the first 24 h of mechanical ventilation, calculated using a previously validated formula. The primary outcome was 30-day mortality. As co-primary analysis, we investigated whether a diagnosis of COVID-19 modified the primary association. We further investigated the association between mechanical power and days being alive and ventilator free and effect modification of this by a diagnosis of COVID-19. Multivariable logistic regression, effect modification and negative binomial regression analyses adjusted for baseline patient characteristics, severity of disease and in-hospital factors, were applied.</p><p><strong>Results: </strong>1,737 mechanically ventilated patients were included, 411 (23.7%) suffered from COVID-19. 509 (29.3%) died within 30 days. The median mechanical power during the first 24 h of ventilation was 19.3 [14.6-24.0] J/min in patients with and 13.2 [10.2-18.0] J/min in patients without COVID-19. A higher mechanical power was associated with 30-day mortality (OR<sub>adj</sub> 1.26 per 1-SD, 7.1J/min increase; 95% CI 1.09-1.46; p = 0.002). Effect modification and interaction analysis did not support that this association was modified by a diagnosis of COVID-19 (95% CI, 0.81-1.38; p-for-interaction = 0.68). A higher mechanical power was associated with a lower number of days alive and ventilator free until day 28 (IRR<sub>adj</sub> 0.83 per 7.1 J/min increase; 95% CI 0.75-0.91; p < 0.001, adjusted risk difference - 2.7 days per 7.1J/min increase; 95% CI - 4.1 to - 1.3).</p><p><strong>Conclusion: </strong>A higher mechanical power is associated with elevated 30-day mortality. While patients with COVID-19 received mechanical ventilation with higher mechanical power, this association was independent of a concomitant diagnosis of COVID-19.</p>","PeriodicalId":16123,"journal":{"name":"Journal of Intensive Care","volume":null,"pages":null},"PeriodicalIF":3.8000,"publicationDate":"2023-04-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10077655/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40560-023-00662-7","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Previous studies linked a high intensity of ventilation, measured as mechanical power, to mortality in patients suffering from "classic" ARDS. By contrast, mechanically ventilated patients with a diagnosis of COVID-19 may present with intact pulmonary mechanics while undergoing mechanical ventilation for longer periods of time. We investigated whether an association between higher mechanical power and mortality is modified by a diagnosis of COVID-19.
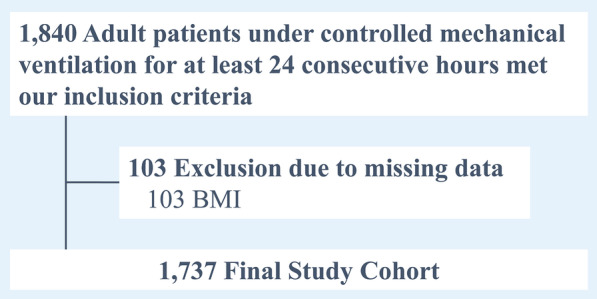
Methods: This retrospective study included critically ill, adult patients who were mechanically ventilated for at least 24 h between March 2020 and December 2021 at a tertiary healthcare facility in Boston, Massachusetts. The primary exposure was median mechanical power during the first 24 h of mechanical ventilation, calculated using a previously validated formula. The primary outcome was 30-day mortality. As co-primary analysis, we investigated whether a diagnosis of COVID-19 modified the primary association. We further investigated the association between mechanical power and days being alive and ventilator free and effect modification of this by a diagnosis of COVID-19. Multivariable logistic regression, effect modification and negative binomial regression analyses adjusted for baseline patient characteristics, severity of disease and in-hospital factors, were applied.
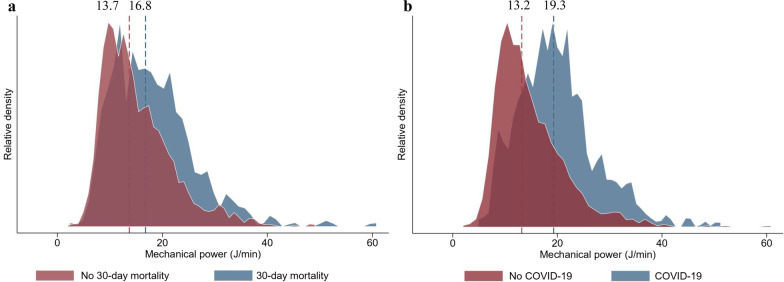
Results: 1,737 mechanically ventilated patients were included, 411 (23.7%) suffered from COVID-19. 509 (29.3%) died within 30 days. The median mechanical power during the first 24 h of ventilation was 19.3 [14.6-24.0] J/min in patients with and 13.2 [10.2-18.0] J/min in patients without COVID-19. A higher mechanical power was associated with 30-day mortality (ORadj 1.26 per 1-SD, 7.1J/min increase; 95% CI 1.09-1.46; p = 0.002). Effect modification and interaction analysis did not support that this association was modified by a diagnosis of COVID-19 (95% CI, 0.81-1.38; p-for-interaction = 0.68). A higher mechanical power was associated with a lower number of days alive and ventilator free until day 28 (IRRadj 0.83 per 7.1 J/min increase; 95% CI 0.75-0.91; p < 0.001, adjusted risk difference - 2.7 days per 7.1J/min increase; 95% CI - 4.1 to - 1.3).
Conclusion: A higher mechanical power is associated with elevated 30-day mortality. While patients with COVID-19 received mechanical ventilation with higher mechanical power, this association was independent of a concomitant diagnosis of COVID-19.
期刊介绍:
"Journal of Intensive Care" is an open access journal dedicated to the comprehensive coverage of intensive care medicine, providing a platform for the latest research and clinical insights in this critical field. The journal covers a wide range of topics, including intensive and critical care, trauma and surgical intensive care, pediatric intensive care, acute and emergency medicine, perioperative medicine, resuscitation, infection control, and organ dysfunction.
Recognizing the importance of cultural diversity in healthcare practices, "Journal of Intensive Care" also encourages submissions that explore and discuss the cultural aspects of intensive care, aiming to promote a more inclusive and culturally sensitive approach to patient care. By fostering a global exchange of knowledge and expertise, the journal contributes to the continuous improvement of intensive care practices worldwide.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


