Bridget L Ryan, Luke Mondor, Walter P Wodchis, Richard H Glazier, Leslie Meredith, Martin Fortin, Moira Stewart
{"title":"Effect of a multimorbidity intervention on health care utilization and costs in Ontario: randomized controlled trial and propensity-matched analyses.","authors":"Bridget L Ryan, Luke Mondor, Walter P Wodchis, Richard H Glazier, Leslie Meredith, Martin Fortin, Moira Stewart","doi":"10.9778/cmajo.20220006","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with multimorbidity require coordinated and patient-centred care. Telemedicine IMPACT Plus provides such care for complex patients in Toronto, Ontario. We conducted a randomized controlled trial (RCT) comparing health care utilization and costs at 1-year postintervention for an intervention group and 2 control groups (RCT and propensity matched).</p><p><strong>Methods: </strong>Data for 82 RCT intervention and 74 RCT control participants were linked with health administrative data. We created a second control group using health administrative data-derived propensity scores to match (1:5) intervention participants with comparators. We evaluated 5 outcomes: acute hospital admissions, emergency department visits, costs of all insured health care, 30-day hospital readmissions and 7-day family physician follow-up after hospital discharge using generalized linear models for RCT controls and generalized estimating equations for propensity-matched controls.</p><p><strong>Results: </strong>There were no significant differences between intervention participants and either control group. For hospital admissions, emergency department visits, costs and readmissions, the relative differences ranged from 1.00 (95% confidence interval [CI] 0.39-2.60) to 1.67 (95% CI 0.82-3.38) with intervention costs at about Can$20 000, RCT controls costs at around Can$15 000 and propensity controls costs at around Can$17 000. There was a higher rate of follow-up with a family physician for the intervention participants compared with the RCT controls (53.13 v. 21.43 per 100 hospital discharges; relative difference 2.48 [95% CI 0.98-6.29]) and propensity-matched controls (49.94 v. 28.21 per 100 hospital discharges; relative difference 1.81 [95% CI 0.99-3.30]).</p><p><strong>Interpretation: </strong>Despite a complex patient-centred intervention, there was no significant improvement in health care utilization or cost. Future research requires larger sample sizes and should include outcomes important to patients and the health care system, and longer follow-up periods.</p><p><strong>Ontario: </strong>ClinicalTrials.gov : 104191.</p>","PeriodicalId":10432,"journal":{"name":"CMAJ open","volume":"11 1","pages":"E45-E53"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/72/55/cmajo.20220006.PMC9851625.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CMAJ open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.9778/cmajo.20220006","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Patients with multimorbidity require coordinated and patient-centred care. Telemedicine IMPACT Plus provides such care for complex patients in Toronto, Ontario. We conducted a randomized controlled trial (RCT) comparing health care utilization and costs at 1-year postintervention for an intervention group and 2 control groups (RCT and propensity matched).
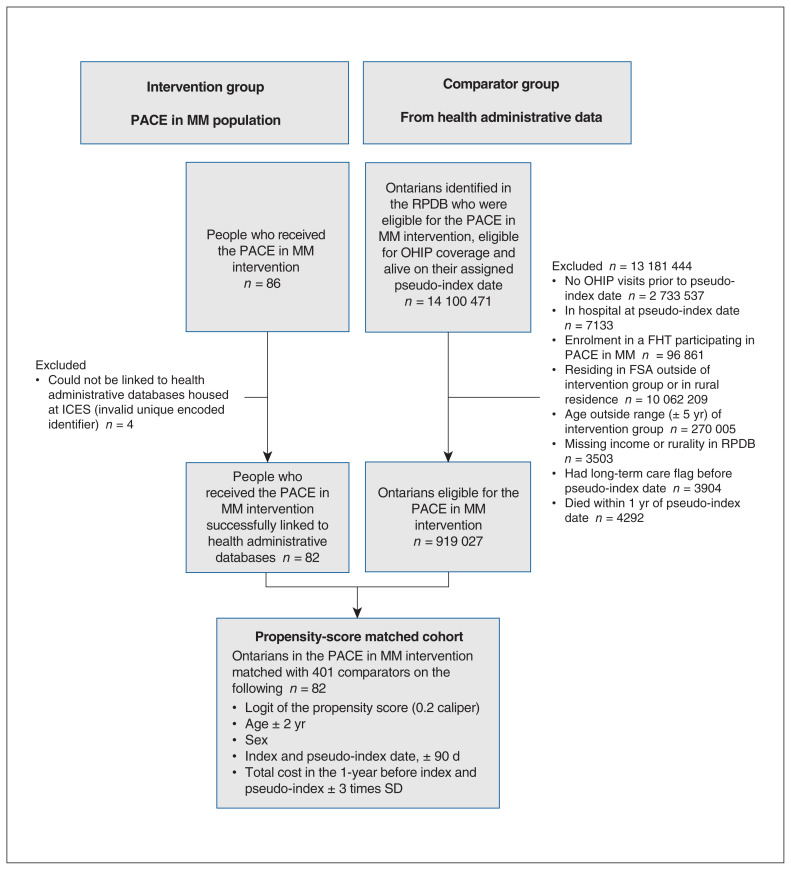
Methods: Data for 82 RCT intervention and 74 RCT control participants were linked with health administrative data. We created a second control group using health administrative data-derived propensity scores to match (1:5) intervention participants with comparators. We evaluated 5 outcomes: acute hospital admissions, emergency department visits, costs of all insured health care, 30-day hospital readmissions and 7-day family physician follow-up after hospital discharge using generalized linear models for RCT controls and generalized estimating equations for propensity-matched controls.
Results: There were no significant differences between intervention participants and either control group. For hospital admissions, emergency department visits, costs and readmissions, the relative differences ranged from 1.00 (95% confidence interval [CI] 0.39-2.60) to 1.67 (95% CI 0.82-3.38) with intervention costs at about Can$20 000, RCT controls costs at around Can$15 000 and propensity controls costs at around Can$17 000. There was a higher rate of follow-up with a family physician for the intervention participants compared with the RCT controls (53.13 v. 21.43 per 100 hospital discharges; relative difference 2.48 [95% CI 0.98-6.29]) and propensity-matched controls (49.94 v. 28.21 per 100 hospital discharges; relative difference 1.81 [95% CI 0.99-3.30]).
Interpretation: Despite a complex patient-centred intervention, there was no significant improvement in health care utilization or cost. Future research requires larger sample sizes and should include outcomes important to patients and the health care system, and longer follow-up periods.
背景:多病患者需要协调和以患者为中心的护理。远程医疗IMPACT Plus为安大略省多伦多的复杂患者提供此类护理。我们进行了一项随机对照试验(RCT),比较干预组和2个对照组(RCT和倾向匹配)干预后1年的医疗保健利用和费用。方法:将82名RCT干预组和74名RCT对照组的数据与卫生管理数据相关联。我们创建了第二个对照组,使用健康管理数据衍生的倾向得分来匹配(1:5)干预参与者与比较者。我们评估了5个结局:急性住院、急诊科就诊、所有参保医疗保健费用、出院后30天再入院和7天家庭医生随访,使用RCT对照的广义线性模型和倾向匹配对照的广义估计方程。结果:干预组与对照组之间无显著差异。对于住院、急诊科就诊、费用和再入院,相对差异范围为1.00(95%置信区间[CI] 0.39-2.60)至1.67 (95% CI 0.82-3.38),干预成本约为20,000加元,RCT控制成本约为15,000加元,倾向控制成本约为17,000加元。与RCT对照组相比,干预组接受家庭医生随访的比例更高(53.13 vs 21.43 / 100;相对差异2.48 [95% CI 0.98-6.29])和倾向匹配对照(49.94 vs 28.21 / 100次出院;相对差异1.81 [95% CI 0.99-3.30])。解释:尽管采取了复杂的以患者为中心的干预措施,但在医疗保健利用或成本方面没有显著改善。未来的研究需要更大的样本量,并应包括对患者和卫生保健系统重要的结果,以及更长的随访期。安大略省:ClinicalTrials.gov: 104191。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


