Cost-effectiveness modelling of birth and infant dose vaccination against hepatitis B virus in Ontario from 2020 to 2050.
引用次数: 1
Abstract
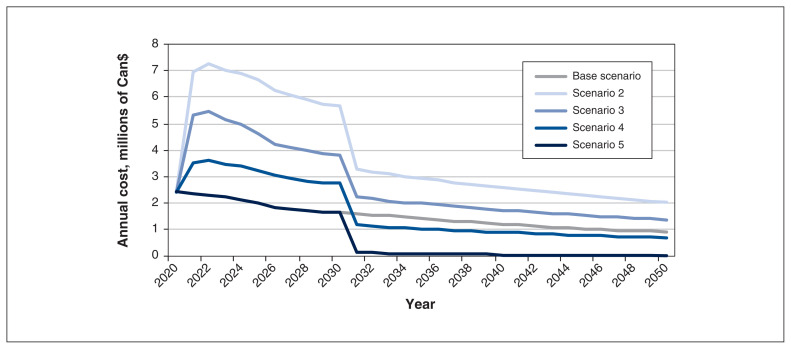
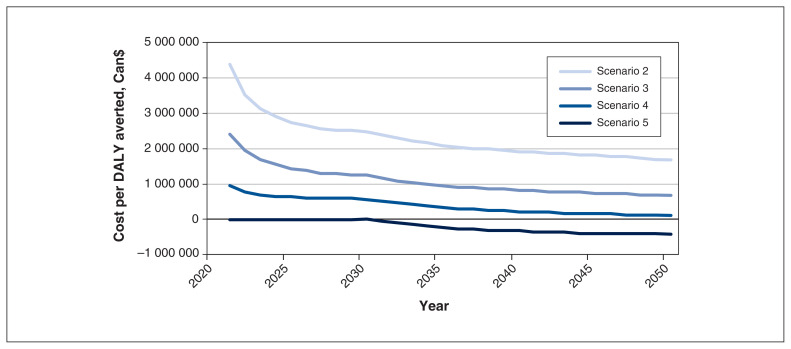
Background: The World Health Organization recommends universal birth dose vaccination for hepatitis B virus (HBV), yet only 3 provinces and territories in Canada provide birth dose vaccination, and Canadian-born children in Ontario are acquiring HBV before adolescent vaccination. We sought to determine whether birth and/or infant HBV vaccination is cost-effective. Methods: We used a dynamic HBV model that incorporates population by year, disease stage, sex and the influence of immigration to quantify the disease and economic burden of chronic HBV infection in Ontario from 2020 to 2050. We compared 4 vaccination scenarios, which included a birth dose vaccine and variations of the 2 subsequent doses (either alone or as a part of the hexavalent vaccine) and a hexavalent-only strategy in infancy with the current adolescent vaccination strategy. Our costing estimates were based on values from 2020. Results: All 4 infant vaccination approaches prevented an additional 550–560 acute and 160 chronic pediatric HBV infections from 2020 to 2050 compared with adolescent vaccination. Whereas birth dose could be cost-effective, incorporating vaccination into a hexavalent vaccine was cost saving. By 2050, the hexavalent approach led to $428 000 in cost savings per disability-adjusted life years averted. Interpretation: At the current prevalence in Ontario, a switch to birth dose or infant dose will be cost-effective or even cost saving. Introducing any form of infant HBV immunization in Ontario will prevent acute and chronic pediatric HBV infections.
2020年至2050年安大略省出生和婴儿接种乙型肝炎病毒疫苗的成本效益模型。
背景:世界卫生组织建议普遍接种出生剂量乙型肝炎病毒(HBV)疫苗,但加拿大只有3个省和地区提供出生剂量疫苗接种,安大略省的加拿大出生儿童在青少年接种疫苗之前获得HBV。我们试图确定出生和/或婴儿乙肝疫苗接种是否具有成本效益。方法:采用纳入按年份、疾病分期、性别和移民影响的动态HBV模型,量化安大略省2020 - 2050年慢性HBV感染的疾病和经济负担。我们比较了4种疫苗接种方案,其中包括出生剂量疫苗和随后两种剂量的变化(单独或作为六价疫苗的一部分),以及婴儿期仅六价疫苗接种策略与当前青少年疫苗接种策略。我们的成本估算是基于2020年的价值。结果:与青少年疫苗接种相比,所有4种婴儿疫苗接种方法在2020年至2050年期间预防了550-560例急性和160例慢性儿科HBV感染。虽然出生剂量可能具有成本效益,但将疫苗接种纳入六价疫苗可以节省成本。到2050年,六价方法导致每个避免残疾调整生命年的成本节省42.8万美元。解释:根据安大略省目前的流行情况,改用出生剂量或婴儿剂量将具有成本效益,甚至可以节省成本。在安大略省引入任何形式的婴儿乙肝病毒免疫将预防急性和慢性儿科乙肝病毒感染。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


