Ellen C Rowlands Snyder, Elspeth McGregor, Doug Coyle
{"title":"Universal ophthalmia neonatorum prophylaxis in Ontario: a cost-effectiveness analysis.","authors":"Ellen C Rowlands Snyder, Elspeth McGregor, Doug Coyle","doi":"10.9778/cmajo.20210226","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Although prophylaxis for ophthalmia neonatorum at birth is required by law in Ontario, declining prevalence of disease and efficacy of prophylaxis have called this practice into question. The objective of this modelling study was to assess the cost-effectiveness of universal prophylaxis for ophthalmia neonatorum to inform decision-makers on the potential impact of a change in this policy.</p><p><strong>Methods: </strong>We compared the cost-effectiveness of prophylaxis for ophthalmia neonatorum with no prophylaxis through cost-utility analysis with a lifetime time horizon, considering a provincial government payer, for a hypothetical population of newborns in Ontario. We assessed both the mean incremental costs of prophylaxis and its mean incremental effectiveness using a hybrid (part decision tree, part Markov) model. We used a scenario analysis to evaluate alternative time horizons and discount rates. We conducted a threshold analysis to evaluate the impact of variations in the cost of prophylaxis and in the prevalence of sexually transmitted infections (gonorrhea and chlamydia).</p><p><strong>Results: </strong>In our model, prophylaxis for ophthalmia neonatorum did not meet a willingness-to-pay threshold of Can$50 000 per quality-adjusted life-year (QALY). Although prophylaxis was effective in reducing morbidity associated with ophthalmia neonatorum, the number needed to treat to prevent 1 case of ophthalmia neonatorum blindness was 500 000, with an associated cost of more than Can$4 000 000. When compared with no prophylaxis, prophylaxis had an incremental cost of Can$355 798 per long-term QALY gained (incremental cost-effectiveness ratio).</p><p><strong>Interpretation: </strong>We found that prophylaxis for ophthalmia neonatorum, although individually inexpensive, leads to very high costs on a population level. These findings contribute to the discussion on mandatory prophylaxis currently underway in several jurisdictions.</p>","PeriodicalId":10432,"journal":{"name":"CMAJ open","volume":"11 1","pages":"E33-E39"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d4/8f/cmajo.20210226.PMC9851624.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CMAJ open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.9778/cmajo.20210226","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Although prophylaxis for ophthalmia neonatorum at birth is required by law in Ontario, declining prevalence of disease and efficacy of prophylaxis have called this practice into question. The objective of this modelling study was to assess the cost-effectiveness of universal prophylaxis for ophthalmia neonatorum to inform decision-makers on the potential impact of a change in this policy.
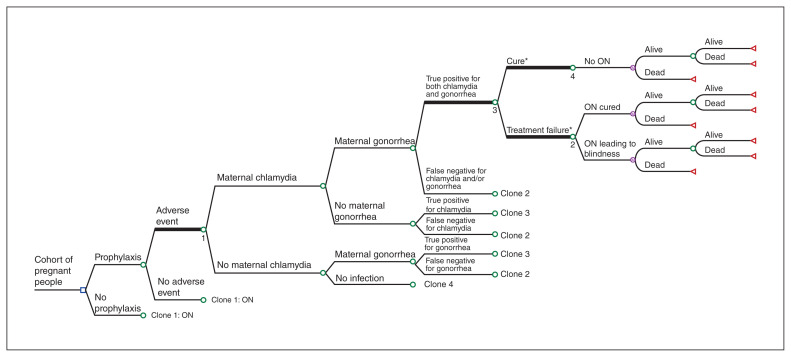
Methods: We compared the cost-effectiveness of prophylaxis for ophthalmia neonatorum with no prophylaxis through cost-utility analysis with a lifetime time horizon, considering a provincial government payer, for a hypothetical population of newborns in Ontario. We assessed both the mean incremental costs of prophylaxis and its mean incremental effectiveness using a hybrid (part decision tree, part Markov) model. We used a scenario analysis to evaluate alternative time horizons and discount rates. We conducted a threshold analysis to evaluate the impact of variations in the cost of prophylaxis and in the prevalence of sexually transmitted infections (gonorrhea and chlamydia).
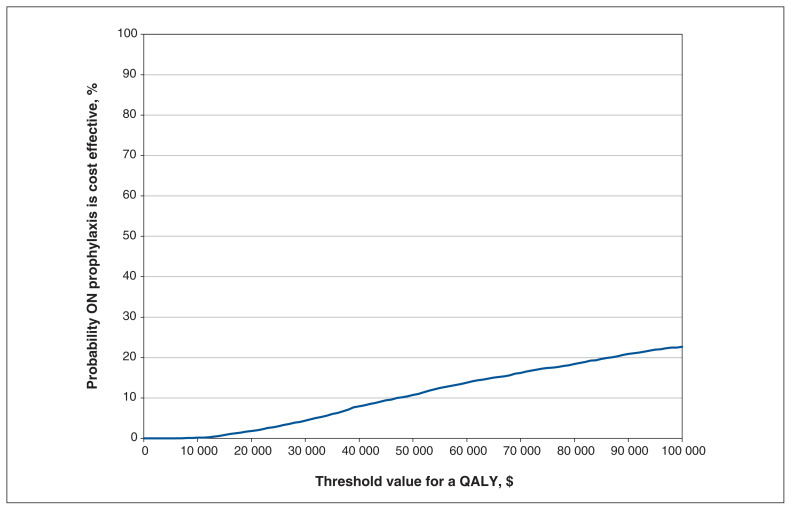
Results: In our model, prophylaxis for ophthalmia neonatorum did not meet a willingness-to-pay threshold of Can$50 000 per quality-adjusted life-year (QALY). Although prophylaxis was effective in reducing morbidity associated with ophthalmia neonatorum, the number needed to treat to prevent 1 case of ophthalmia neonatorum blindness was 500 000, with an associated cost of more than Can$4 000 000. When compared with no prophylaxis, prophylaxis had an incremental cost of Can$355 798 per long-term QALY gained (incremental cost-effectiveness ratio).
Interpretation: We found that prophylaxis for ophthalmia neonatorum, although individually inexpensive, leads to very high costs on a population level. These findings contribute to the discussion on mandatory prophylaxis currently underway in several jurisdictions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


