Mona Abdel-Halim Ibrahim, Nada Eltayeb, Mirna Michel Ibrahim, Ahmed Nassar, Maged Daruish, Maha El-Zimaity, Mahmoud El-Lithy, Ahmed Mostafa, Amal El-Afifi, Haitham Abdelbary, Mahira Hamdy El-Sayed
{"title":"Suggested Guidelines for the Treatment of Mycosis Fungoides in Countries with Limited Resources.","authors":"Mona Abdel-Halim Ibrahim, Nada Eltayeb, Mirna Michel Ibrahim, Ahmed Nassar, Maged Daruish, Maha El-Zimaity, Mahmoud El-Lithy, Ahmed Mostafa, Amal El-Afifi, Haitham Abdelbary, Mahira Hamdy El-Sayed","doi":"10.1155/2023/1360740","DOIUrl":null,"url":null,"abstract":"<p><p>The treatment options for mycosis fungoides (MF) have been expanding but unfortunately many of the currently used treatment modalities are unavailable in Egypt and other African/Arab countries. In addition, there is a lack of consensus on the treatment of hypopigmented MF (HMF), which is a frequently encountered variant in our population. We aimed to develop regional treatment guidelines based on the international guidelines but modified to encompass the restricted treatment availability and our institutional experience. Special attention was also given to studies conducted on patients with skin phototype (III-IV). Treatment algorithm was formulated at Ain-Shams cutaneous lymphoma clinic through the collaboration of dermatologists, haematologists, and oncologists. Level of evidence is specified for each treatment option. For HMF, phototherapy is recommended as a first line treatment, while low-dose methotrexate is considered a second line. For early classical MF, we recommend Psoralen-ultraviolet A (PUVA), which is a well-tolerated treatment option in dark phenotype. Addition of either retinoic acid receptor (RAR) agonist and/or methotrexate is recommended as a second line. Total skin electron beam (TSEB) is considered a third-line option. For advanced stage, PUVA plus RAR agonist and/or methotrexate is recommended as first line, TSEB or monochemotherapy is considered a second line option. Polychemotherapy is regarded as a final option. All patients with complete response (CR) enter a maintenance and follow-up schedule. We suggest a practical algorithm for the treatment of MF for patients with dark phenotype living in countries with limited resources.</p>","PeriodicalId":11338,"journal":{"name":"Dermatology Research and Practice","volume":"2023 ","pages":"1360740"},"PeriodicalIF":1.5000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9904957/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Dermatology Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2023/1360740","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"DERMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
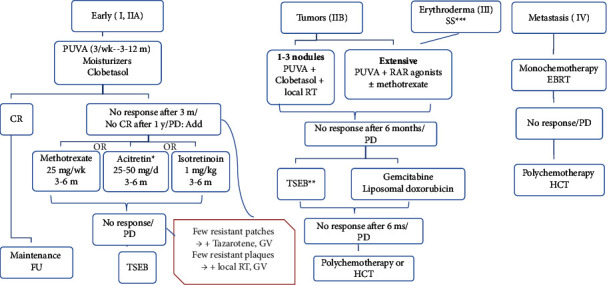
The treatment options for mycosis fungoides (MF) have been expanding but unfortunately many of the currently used treatment modalities are unavailable in Egypt and other African/Arab countries. In addition, there is a lack of consensus on the treatment of hypopigmented MF (HMF), which is a frequently encountered variant in our population. We aimed to develop regional treatment guidelines based on the international guidelines but modified to encompass the restricted treatment availability and our institutional experience. Special attention was also given to studies conducted on patients with skin phototype (III-IV). Treatment algorithm was formulated at Ain-Shams cutaneous lymphoma clinic through the collaboration of dermatologists, haematologists, and oncologists. Level of evidence is specified for each treatment option. For HMF, phototherapy is recommended as a first line treatment, while low-dose methotrexate is considered a second line. For early classical MF, we recommend Psoralen-ultraviolet A (PUVA), which is a well-tolerated treatment option in dark phenotype. Addition of either retinoic acid receptor (RAR) agonist and/or methotrexate is recommended as a second line. Total skin electron beam (TSEB) is considered a third-line option. For advanced stage, PUVA plus RAR agonist and/or methotrexate is recommended as first line, TSEB or monochemotherapy is considered a second line option. Polychemotherapy is regarded as a final option. All patients with complete response (CR) enter a maintenance and follow-up schedule. We suggest a practical algorithm for the treatment of MF for patients with dark phenotype living in countries with limited resources.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


