Anorectal Endoscopic Hybrid Resection of an Uncommon Cause of Debilitating Diarrhoea: Polypoid Supra-Anal Mucosal Prolapse Syndrome.
IF 1
Q4 GASTROENTEROLOGY & HEPATOLOGY
引用次数: 0
Abstract
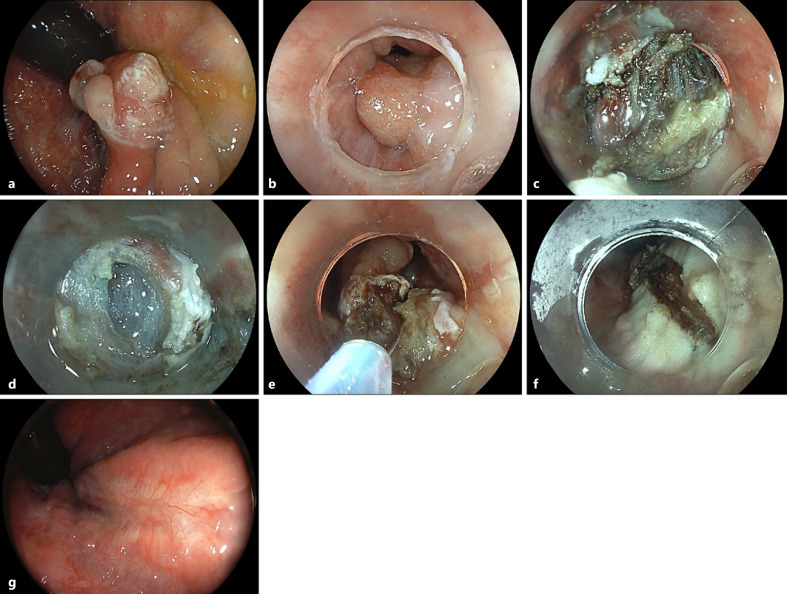
Endoscopic resection of supra-anal lesions is challenging due to marked fibrosis and generous venous plexus [1]. Furthermore, abundance of sensory nerve fibres in the anal canal calls for an adequate local anaesthesia otherwise not warranted in endoscopy [2]. This is the case of a 54-year-old male patient with a 2-year history of debilitating diarrhoea including inability to work (sic!), passing up to 25 watery stools with urgency. Prior gastroenterology consultations elsewhere including previous ileocolonoscopy did not indicate the cause of diarrhoea. Currently, the patient was scheduled for endoscopic resection of an estimated 15-mm, biopsy-confirmed mucosal prolapse polyp in the supra-anal rectum involving the dentate line. The retroflexed endoscopic visualization revealed a reddened polypoid lesion with an eroded surface, consistent with mucosal prolapse syndrome (Fig. 1a). For resection, a cap-fitted, antegrade endoscopic approach was chosen to first isolate the lesion from the squamous epithelium of the anal canal, which indeed was cut into in its proximal aspects after injection of an indigocarmine saline mixture without adrenaline and a local anaesthetic (Fig. 1b). To this end, limited endoscopic submucosal dissection using a Dual Knife J (Olympus, Hamburg, Germany) was performed under deep sedation using propofol and midazolam to ensure wide-margin resection at the anal side with diarrhoea most likely attributable to chronic sphincter irritation (Fig. 1c; note marked fibrosis and prominent vessels). Only after progression to the more oral rectum did the submucosal space begin to open up adequately (Fig. 1d). To accelerate the procedure and with a view to the benign histology, we subsequently opted for a hybrid approach ensnaring the lesion (30-mm snare; Medwork, Höchstadt, Germany) after adequate trimming of the anal parts of the lesion (Fig. 1e). The final resection bed was without bleeding;
肛门直肠内窥镜混合切除一种罕见的导致衰弱性腹泻的原因:息肉样肛上粘膜脱垂综合征。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

GE Portuguese Journal of Gastroenterology
GASTROENTEROLOGY & HEPATOLOGY-
CiteScore
1.60
自引率
11.10%
发文量
62
审稿时长
21 weeks
期刊介绍:
The ''GE Portuguese Journal of Gastroenterology'' (formerly Jornal Português de Gastrenterologia), founded in 1994, is the official publication of Sociedade Portuguesa de Gastrenterologia (Portuguese Society of Gastroenterology), Sociedade Portuguesa de Endoscopia Digestiva (Portuguese Society of Digestive Endoscopy) and Associação Portuguesa para o Estudo do Fígado (Portuguese Association for the Study of the Liver). The journal publishes clinical and basic research articles on Gastroenterology, Digestive Endoscopy, Hepatology and related topics. Review articles, clinical case studies, images, letters to the editor and other articles such as recommendations or papers on gastroenterology clinical practice are also considered. Only articles written in English are accepted.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


