Roland Paulus, Matthias Leonhard, Guan-Yuh Ho, Annabella Kurz, Berit Schneider-Stickler
{"title":"Differences in Glottal Closure and Visibility of the Anterior Commissure during Rigid-90°, Rigid-70°, and Flexible Laryngostroboscopy.","authors":"Roland Paulus, Matthias Leonhard, Guan-Yuh Ho, Annabella Kurz, Berit Schneider-Stickler","doi":"10.1159/000530454","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The conventional rigid-90° and rigid-70° laryngostroboscopy has been so far considered the gold standard in assessing the vibratory behavior of the vocal folds and the glottal closure configuration during phonation. Meanwhile, this rigid laryngostroboscopy is more and more replaced by flexible chip-on-tip systems. The aim of this study was to evaluate the influence of these different endoscopic techniques on glottal closure configuration and on visibility of the complete focal fold length including anterior commissure during phonation.</p><p><strong>Methods: </strong>Twenty-one euphonic subjects were enrolled (mean age 34.6 ± 9.5; m = 10, f = 11). They were examined with the three laryngoscopic techniques (conventional rigid-90°, rigid-70°, and flexible chip-on-tip laryngoscopy during low and high voice pitch with soft and loud voice intensity). For evaluating the degree of glottal closure, a modified classification of Södersten et al. was applied and the visibility of the anterior commissure was evaluated. The correlation of the three endoscopic techniques was assessed with Cohen and Fleiss' kappa.</p><p><strong>Results: </strong>In even low loud phonation, the rigid-90° and rigid-70° endoscopies revealed a complete closure of the glottis in only 47.6% of subjects but with flexible endoscopy in 81%. The complete vocal fold length with anterior commissure was best visible with flexible endoscopy in 90.5% in low-soft and high-soft phonation. The rigid-90° endoscopy showed a slight agreement in comparison with the flexible endoscopy in regard to the types of vocal fold closure with a Cohen's kappa coefficient k = 0.199. The rigid-90° endoscopy showed an almost perfect agreement with k = 0.84 when compared to the rigid-70° endoscopy. The flexible endoscopy compared to the rigid-70° endoscopy showed a fair agreement with k = 0.346.</p><p><strong>Conclusion: </strong>We found mainly corresponding results in both rigid-90° and rigid-70° endoscopic techniques which can be explained by the same transoral approach with the tongue pulled out, whereas the flexible transnasal endoscopy mainly gives a better view on the anterior commissure. The influence of transorally or transnasally guided endoscopic techniques needs to be considered in interpretation of laryngostroboscopic parameters like vocal fold closure and supraglottal hyperactivity.</p>","PeriodicalId":12114,"journal":{"name":"Folia Phoniatrica et Logopaedica","volume":null,"pages":null},"PeriodicalIF":1.1000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10614229/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Folia Phoniatrica et Logopaedica","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000530454","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/3/31 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"AUDIOLOGY & SPEECH-LANGUAGE PATHOLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
Introduction: The conventional rigid-90° and rigid-70° laryngostroboscopy has been so far considered the gold standard in assessing the vibratory behavior of the vocal folds and the glottal closure configuration during phonation. Meanwhile, this rigid laryngostroboscopy is more and more replaced by flexible chip-on-tip systems. The aim of this study was to evaluate the influence of these different endoscopic techniques on glottal closure configuration and on visibility of the complete focal fold length including anterior commissure during phonation.
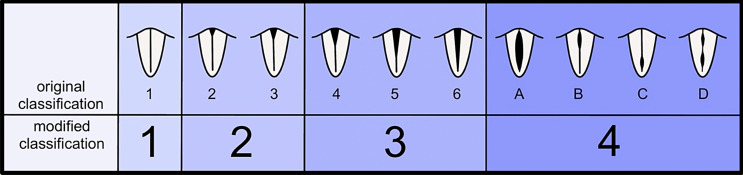
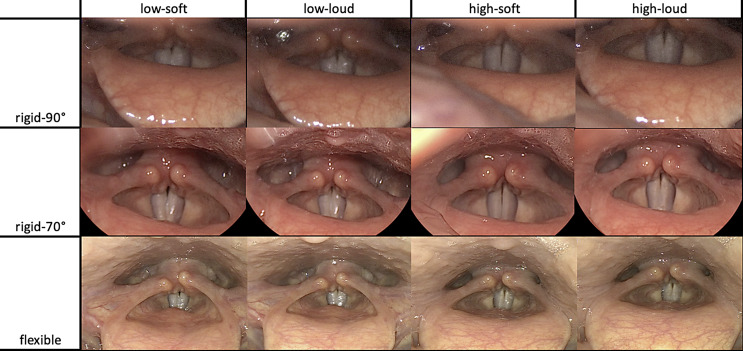
Methods: Twenty-one euphonic subjects were enrolled (mean age 34.6 ± 9.5; m = 10, f = 11). They were examined with the three laryngoscopic techniques (conventional rigid-90°, rigid-70°, and flexible chip-on-tip laryngoscopy during low and high voice pitch with soft and loud voice intensity). For evaluating the degree of glottal closure, a modified classification of Södersten et al. was applied and the visibility of the anterior commissure was evaluated. The correlation of the three endoscopic techniques was assessed with Cohen and Fleiss' kappa.
Results: In even low loud phonation, the rigid-90° and rigid-70° endoscopies revealed a complete closure of the glottis in only 47.6% of subjects but with flexible endoscopy in 81%. The complete vocal fold length with anterior commissure was best visible with flexible endoscopy in 90.5% in low-soft and high-soft phonation. The rigid-90° endoscopy showed a slight agreement in comparison with the flexible endoscopy in regard to the types of vocal fold closure with a Cohen's kappa coefficient k = 0.199. The rigid-90° endoscopy showed an almost perfect agreement with k = 0.84 when compared to the rigid-70° endoscopy. The flexible endoscopy compared to the rigid-70° endoscopy showed a fair agreement with k = 0.346.
Conclusion: We found mainly corresponding results in both rigid-90° and rigid-70° endoscopic techniques which can be explained by the same transoral approach with the tongue pulled out, whereas the flexible transnasal endoscopy mainly gives a better view on the anterior commissure. The influence of transorally or transnasally guided endoscopic techniques needs to be considered in interpretation of laryngostroboscopic parameters like vocal fold closure and supraglottal hyperactivity.
期刊介绍:
Published since 1947, ''Folia Phoniatrica et Logopaedica'' provides a forum for international research on the anatomy, physiology, and pathology of structures of the speech, language, and hearing mechanisms. Original papers published in this journal report new findings on basic function, assessment, management, and test development in communication sciences and disorders, as well as experiments designed to test specific theories of speech, language, and hearing function. Review papers of high quality are also welcomed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


