{"title":"Аre Multivisceral Resections for Gastric Cancer Acceptable: Experience from a High Volume Center and Extended Literature Review?","authors":"Nikola Vladov, Tsvetan Trichkov, Vassil Mihaylov, Ivelin Takorov, Radoslav Kostadinov, Tsonka Lukanova","doi":"10.1055/s-0043-1761278","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction</b> Multivisceral resections (MVRs) in gastric cancer are potentially curable in selected patients in whom clear resection margins are possible. However, there are still uncertain data on their feasibility and safety considering short- and long-term results. The study compares survival, morbidity, mortality, and other secondary outcomes between standard and MVRs for gastric cancer. <b>Materials and Methods</b> A monocentric retrospective study in patients with gastric adenocarcinoma, covering 2004 to 2020. Of the 336 operable cases, 101 patients underwent MVRs. The remaining 235 underwent standard gastric resections (SGRs), of which 173 patients were in stage T3/T4. To compare survival, a control group of 101 patients with palliative procedures was used-bypass anastomosis or exploration. <b>Results</b> MVR had a lower survival rate than the SGR but significantly higher than the palliative procedures. The predominant gender in MVR was male (72.3%), with a mean age of 61 years. The perioperative mortality was 3.96% ( <i>n</i> = 4), and the overall median survival was 28.1 months. The most frequently resected organs were the spleen (67.3%), followed by the pancreas (32.7%) and the liver (20.8%). In 56.4% of the cases two organs were resected, in 28.7% three organs, and in 13.9% four organs. The main complication was bleeding (9.9%). The major postoperative complications in the MVR were 14.85%, and in the SGR 6.4% ( <i>p</i> < 0.05). Better long-term results were observed in patients who underwent R0 resections compared with R1. <b>Conclusion</b> Multiorgan resections are characterized by poorer survival and a higher complication rate than gastrectomies. On the other hand, they have better long-term outcomes than palliative procedures. However, MVRs are admissible when performed by an experienced surgical team in high-volume centers.</p>","PeriodicalId":74891,"journal":{"name":"","volume":"9 1","pages":"e28-e35"},"PeriodicalIF":0.0,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9897905/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0043-1761278","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
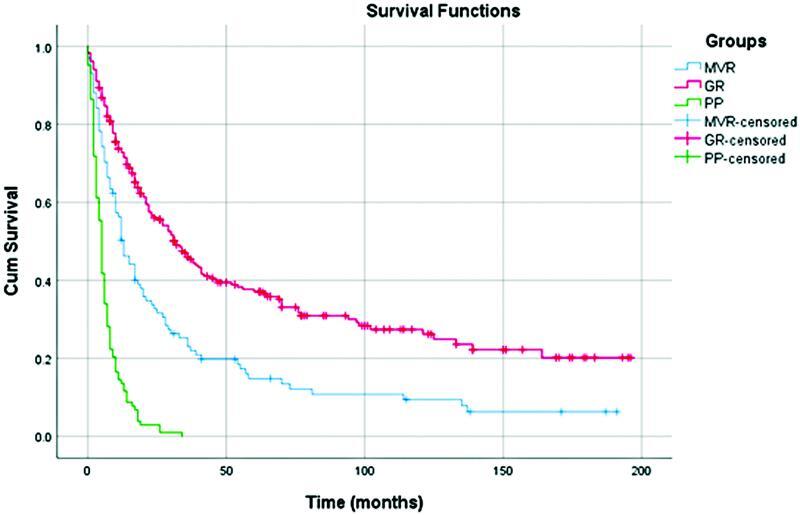
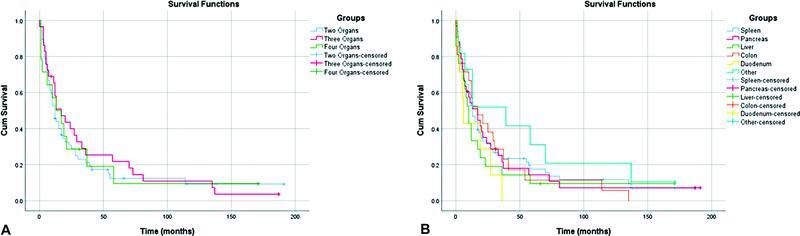
Introduction Multivisceral resections (MVRs) in gastric cancer are potentially curable in selected patients in whom clear resection margins are possible. However, there are still uncertain data on their feasibility and safety considering short- and long-term results. The study compares survival, morbidity, mortality, and other secondary outcomes between standard and MVRs for gastric cancer. Materials and Methods A monocentric retrospective study in patients with gastric adenocarcinoma, covering 2004 to 2020. Of the 336 operable cases, 101 patients underwent MVRs. The remaining 235 underwent standard gastric resections (SGRs), of which 173 patients were in stage T3/T4. To compare survival, a control group of 101 patients with palliative procedures was used-bypass anastomosis or exploration. Results MVR had a lower survival rate than the SGR but significantly higher than the palliative procedures. The predominant gender in MVR was male (72.3%), with a mean age of 61 years. The perioperative mortality was 3.96% ( n = 4), and the overall median survival was 28.1 months. The most frequently resected organs were the spleen (67.3%), followed by the pancreas (32.7%) and the liver (20.8%). In 56.4% of the cases two organs were resected, in 28.7% three organs, and in 13.9% four organs. The main complication was bleeding (9.9%). The major postoperative complications in the MVR were 14.85%, and in the SGR 6.4% ( p < 0.05). Better long-term results were observed in patients who underwent R0 resections compared with R1. Conclusion Multiorgan resections are characterized by poorer survival and a higher complication rate than gastrectomies. On the other hand, they have better long-term outcomes than palliative procedures. However, MVRs are admissible when performed by an experienced surgical team in high-volume centers.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


