Successful treatment of renal malakoplakia via the reduction of immunosuppression and antimicrobial therapy after kidney transplantation: a case report.
Seung Hyuk Yim, Eun-Ki Min, Hyun Jeong Kim, Beom Jin Lim, Kyu Ha Huh
{"title":"Successful treatment of renal malakoplakia via the reduction of immunosuppression and antimicrobial therapy after kidney transplantation: a case report.","authors":"Seung Hyuk Yim, Eun-Ki Min, Hyun Jeong Kim, Beom Jin Lim, Kyu Ha Huh","doi":"10.4285/kjt.22.0048","DOIUrl":null,"url":null,"abstract":"<p><p>Malakoplakia is a rare, granulomatous disease that usually affects immunocompromised individuals and is generally associated with poor graft and patient survival. We present a case of renal malakoplakia after kidney transplantation (KT). A 33-year-old female patient with chronic kidney disease underwent living-donor KT at Severance Hospital. The patient was administered 375 mg/m<sup>2</sup> rituximab due to high panel reactive antibodies. Immunosuppression was initiated with 1.5 mg/kg anti-thymocyte globulin and intravenous methylprednisolone and maintained with tacrolimus, oral methylprednisolone, and mycophenolate mofetil (MMF). Six months after KT, the patient was hospitalized for a urinary tract infection with an elevated serum creatinine level of 3.14 mg/dL. Renal biopsy revealed malakoplakia involving the renal parenchyma. Upon this diagnosis, the dose of tacrolimus was reduced and MMF was stopped. Fluoroquinolone was used for 16 days, and the trimethoprim/sulfamethoxazole dose was doubled for 6 days. The patient was hospitalized for 3 weeks and closely observed during outpatient visits. Follow-up ultrasonography revealed mass-like lesions of renal malakoplakia, which disappeared 5 months after diagnosis. The serum creatinine level decreased to 1.29 mg/dL 28 months after diagnosis. Our results suggest that renal malakoplakia can be successfully treated by the reduction of immunosuppression and sustained antimicrobial therapy.</p>","PeriodicalId":33357,"journal":{"name":"Korean Journal of Transplantation","volume":"36 4","pages":"289-293"},"PeriodicalIF":0.0000,"publicationDate":"2022-12-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/57/55/kjt-36-4-289.PMC9832590.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Transplantation","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4285/kjt.22.0048","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 2
Abstract
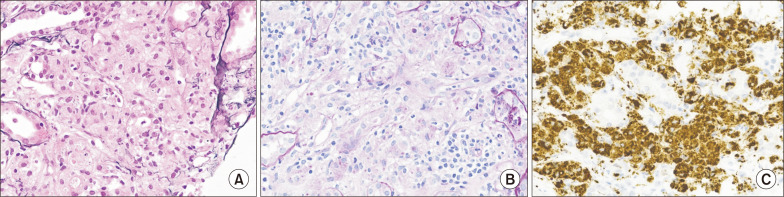
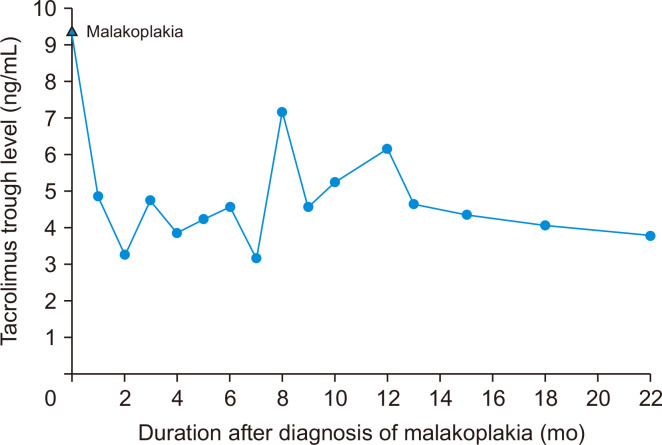
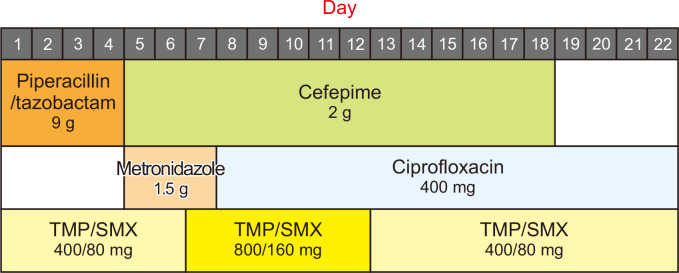
Malakoplakia is a rare, granulomatous disease that usually affects immunocompromised individuals and is generally associated with poor graft and patient survival. We present a case of renal malakoplakia after kidney transplantation (KT). A 33-year-old female patient with chronic kidney disease underwent living-donor KT at Severance Hospital. The patient was administered 375 mg/m2 rituximab due to high panel reactive antibodies. Immunosuppression was initiated with 1.5 mg/kg anti-thymocyte globulin and intravenous methylprednisolone and maintained with tacrolimus, oral methylprednisolone, and mycophenolate mofetil (MMF). Six months after KT, the patient was hospitalized for a urinary tract infection with an elevated serum creatinine level of 3.14 mg/dL. Renal biopsy revealed malakoplakia involving the renal parenchyma. Upon this diagnosis, the dose of tacrolimus was reduced and MMF was stopped. Fluoroquinolone was used for 16 days, and the trimethoprim/sulfamethoxazole dose was doubled for 6 days. The patient was hospitalized for 3 weeks and closely observed during outpatient visits. Follow-up ultrasonography revealed mass-like lesions of renal malakoplakia, which disappeared 5 months after diagnosis. The serum creatinine level decreased to 1.29 mg/dL 28 months after diagnosis. Our results suggest that renal malakoplakia can be successfully treated by the reduction of immunosuppression and sustained antimicrobial therapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


