{"title":"Radiation Retinopathy after Heavy Ion Particle Therapy for Maxillary Sinus Cancer: A Case Report.","authors":"Choong Man Choi, Se Joon Woo","doi":"10.3341/kjo.2022.0119","DOIUrl":null,"url":null,"abstract":"Dear Editor, Radiation retinopathy (RR) is a delayed obstructive microvascular retinopathy that usually develops months to years after radiation therapy and has characteristic findings, such as intraretinal hemorrhage, cotton wool patches, and capillary nonperfusion. Heavy ion particle therapy (HIPT) has emerged as a new technology owing to its safety. Currently, few cases of RR after HIPT have been reported in Japan [1]. Here, we report the first case of RR after HIPT in South Korea. This report was approved by the Institutional Review Board of Seoul National University Bundang Hospital (No. B-2208-774-706) and the patient provided written informed consent for publication of this case report. A 37-year-old male patient visited the clinic for evaluation of his eye 1 month after receiving a total dose of 70.4 Gy carbon HIPT over 16 fractions in an area that included the optic nerve for undifferentiated polymorphic sarcoma in the right maxillary sinus. Brain and orbital magnetic resonance imaging (MRI) revealed that the tumor was in contact with the medial and inferior rectus muscles but did not invade the eyeball or optic nerve. Dendritic cell-based cancer vaccine treatment was concurrently combined with HIPT. Corrected visual acuity of 20 / 16 in the right eye was measured, and no abnormalities were found in the anterior segment and fundus. After 23 months of HIPT, the corrected visual acuity was 20 / 125 in the right eye. Relative afferent pupillary defect and optic disc pallor were present in the right eye. Although atrophy or inflammation of the optic nerve was not confirmed by MRI, circumferential peripheral visual field defect was present. These were signs of optic neuropathy. Fluorescein angiography and optical coherence tomography (OCT) angiography were performed. There was no retinal neovascularization, but extensive nonperfusion of the peripheral retina including the macular area with multiple intraretinal hemorrhages and cotton wool patches was observed in the right eye (Fig. 1A–1D). Since the choroidal and retinal perfusion times were within normal range, diseases that induce perfusion abnormalities, such as retinal artery occlusion or ocular ischemic syndrome were excluded. Panretinal photocoagulation was performed to prevent neovascular complications. After 33 months of HIPT, the visual-evoked potential revealed decreased P100 amplitude in the right eye which could be explained by both RR and radiation optic neuropathy. Panretinal photocoagulation was additionally performed because of iris neovascularization. After 3 months, the intraocular pressure increased to 24 mmHg with worsening of iris neovascularization in the right eye. Under the diagnosis of neovascular glaucoma, the intraocular pressure-lowering drugs were prescribed. Additionally, intravitreal bevacizumab (Avastin, Roche) was administered to the right eye five times every few months. After 59 months of HIPT, cataract surgery was performed in the right eye for an intumescent cataract (Fig. 1E). Even after cataract surgery, the patient was unable to sense light with the right eye. Slit-lamp examination showed no iris neovascularization. On funduscopic examination, severe optic disc atrophy was observed (Fig. 1F). OCT showed overall retinal thinning and disruption in the right eye (Fig. 1G). Recently, HIPT has been widely used in multiple periorbital cancer for its advantage of “Bragg peak” and “high relative biological effectiveness.” Bragg peak is a feature of particle radiation, delivering its maximum radiation dose to the tumor and minimizing damage to surrounding normal tissue [2]. With the Bragg peak, the occurrence of RR would be low with particle therapy; a previous study confirmed the superiority of particle therapy for RR occurrence [3]. Furthermore, the high relative biological effectiveness of HIPT compared to other radiation therapies enables less radiation to destroy the tumor [4]. Risk factors for the development of RR include total raKorean J Ophthalmol 2023;37(1):88-90 https://doi.org/10.3341/kjo.2022.0119","PeriodicalId":17883,"journal":{"name":"Korean Journal of Ophthalmology : KJO","volume":"37 1","pages":"88-90"},"PeriodicalIF":0.0000,"publicationDate":"2023-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/db/f1/kjo-2022-0119.PMC9935066.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Ophthalmology : KJO","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3341/kjo.2022.0119","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
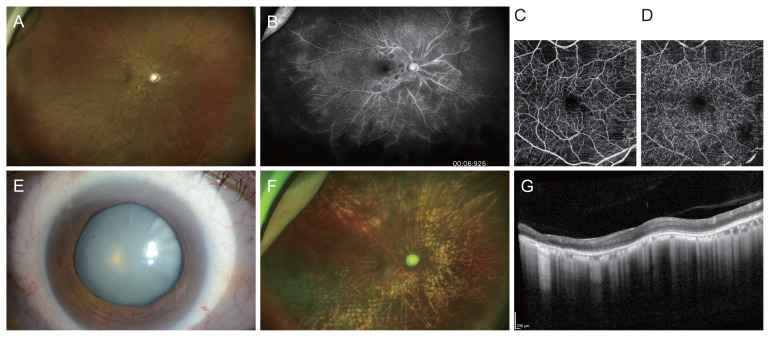
Dear Editor, Radiation retinopathy (RR) is a delayed obstructive microvascular retinopathy that usually develops months to years after radiation therapy and has characteristic findings, such as intraretinal hemorrhage, cotton wool patches, and capillary nonperfusion. Heavy ion particle therapy (HIPT) has emerged as a new technology owing to its safety. Currently, few cases of RR after HIPT have been reported in Japan [1]. Here, we report the first case of RR after HIPT in South Korea. This report was approved by the Institutional Review Board of Seoul National University Bundang Hospital (No. B-2208-774-706) and the patient provided written informed consent for publication of this case report. A 37-year-old male patient visited the clinic for evaluation of his eye 1 month after receiving a total dose of 70.4 Gy carbon HIPT over 16 fractions in an area that included the optic nerve for undifferentiated polymorphic sarcoma in the right maxillary sinus. Brain and orbital magnetic resonance imaging (MRI) revealed that the tumor was in contact with the medial and inferior rectus muscles but did not invade the eyeball or optic nerve. Dendritic cell-based cancer vaccine treatment was concurrently combined with HIPT. Corrected visual acuity of 20 / 16 in the right eye was measured, and no abnormalities were found in the anterior segment and fundus. After 23 months of HIPT, the corrected visual acuity was 20 / 125 in the right eye. Relative afferent pupillary defect and optic disc pallor were present in the right eye. Although atrophy or inflammation of the optic nerve was not confirmed by MRI, circumferential peripheral visual field defect was present. These were signs of optic neuropathy. Fluorescein angiography and optical coherence tomography (OCT) angiography were performed. There was no retinal neovascularization, but extensive nonperfusion of the peripheral retina including the macular area with multiple intraretinal hemorrhages and cotton wool patches was observed in the right eye (Fig. 1A–1D). Since the choroidal and retinal perfusion times were within normal range, diseases that induce perfusion abnormalities, such as retinal artery occlusion or ocular ischemic syndrome were excluded. Panretinal photocoagulation was performed to prevent neovascular complications. After 33 months of HIPT, the visual-evoked potential revealed decreased P100 amplitude in the right eye which could be explained by both RR and radiation optic neuropathy. Panretinal photocoagulation was additionally performed because of iris neovascularization. After 3 months, the intraocular pressure increased to 24 mmHg with worsening of iris neovascularization in the right eye. Under the diagnosis of neovascular glaucoma, the intraocular pressure-lowering drugs were prescribed. Additionally, intravitreal bevacizumab (Avastin, Roche) was administered to the right eye five times every few months. After 59 months of HIPT, cataract surgery was performed in the right eye for an intumescent cataract (Fig. 1E). Even after cataract surgery, the patient was unable to sense light with the right eye. Slit-lamp examination showed no iris neovascularization. On funduscopic examination, severe optic disc atrophy was observed (Fig. 1F). OCT showed overall retinal thinning and disruption in the right eye (Fig. 1G). Recently, HIPT has been widely used in multiple periorbital cancer for its advantage of “Bragg peak” and “high relative biological effectiveness.” Bragg peak is a feature of particle radiation, delivering its maximum radiation dose to the tumor and minimizing damage to surrounding normal tissue [2]. With the Bragg peak, the occurrence of RR would be low with particle therapy; a previous study confirmed the superiority of particle therapy for RR occurrence [3]. Furthermore, the high relative biological effectiveness of HIPT compared to other radiation therapies enables less radiation to destroy the tumor [4]. Risk factors for the development of RR include total raKorean J Ophthalmol 2023;37(1):88-90 https://doi.org/10.3341/kjo.2022.0119

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


