Liqi Shu, Adam de Havenon, Ava L Liberman, Nils Henninger, Eric Goldstein, Michael E Reznik, Ali Mahta, Fawaz Al-Mufti, Jennifer Frontera, Karen Furie, Shadi Yaghi
{"title":"Trends in Venous Thromboembolism Readmission Rates after Ischemic Stroke and Intracerebral Hemorrhage.","authors":"Liqi Shu, Adam de Havenon, Ava L Liberman, Nils Henninger, Eric Goldstein, Michael E Reznik, Ali Mahta, Fawaz Al-Mufti, Jennifer Frontera, Karen Furie, Shadi Yaghi","doi":"10.5853/jos.2022.02215","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and purpose: </strong>Venous thromboembolism (VTE) is a life-threatening complication of stroke. We evaluated nationwide rates and risk factors for hospital readmissions with VTE after an intracerebral hemorrhage (ICH) or acute ischemic stroke (AIS) hospitalization.</p><p><strong>Methods: </strong>Using the Healthcare Cost and Utilization Project (HCUP) Nationwide Readmission Database, we included patients with a principal discharge diagnosis of ICH or AIS from 2016 to 2019. Patients who had VTE diagnosis or history of VTE during the index admission were excluded. We performed Cox regression models to determine factors associated with VTE readmission, compared rates between AIS and ICH and developed post-stroke VTE risk score. We estimated VTE readmission rates per day over a 90-day time window post-discharge using linear splines.</p><p><strong>Results: </strong>Of the total 1,459,865 patients with stroke, readmission with VTE as the principal diagnosis within 90 days occurred in 0.26% (3,407/1,330,584) AIS and 0.65% (843/129,281) ICH patients. The rate of VTE readmission decreased within first 4-6 weeks (P<0.001). In AIS, cancer, obesity, higher National Institutes of Health Stroke Scale (NIHSS) score, longer hospital stay, home or rehabilitation disposition, and absence of atrial fibrillation were associated with VTE readmission. In ICH, longer hospital stay and rehabilitation disposition were associated with VTE readmission. The VTE rate was higher in ICH compared to AIS (adjusted hazard ratio 2.86, 95% confidence interval 1.93-4.25, P<0.001).</p><p><strong>Conclusions: </strong>After stroke, VTE readmission risk is highest within the first 4-6 weeks and nearly three-fold higher after ICH vs. AIS. VTE risk is linked to decreased mobility and hypercoagulability. Studies are needed to test short-term VTE prophylaxis beyond hospitalization in high-risk patients.</p>","PeriodicalId":17135,"journal":{"name":"Journal of Stroke","volume":"25 1","pages":"151-159"},"PeriodicalIF":6.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/09/af/jos-2022-02215.PMC9911841.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Stroke","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5853/jos.2022.02215","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and purpose: Venous thromboembolism (VTE) is a life-threatening complication of stroke. We evaluated nationwide rates and risk factors for hospital readmissions with VTE after an intracerebral hemorrhage (ICH) or acute ischemic stroke (AIS) hospitalization.
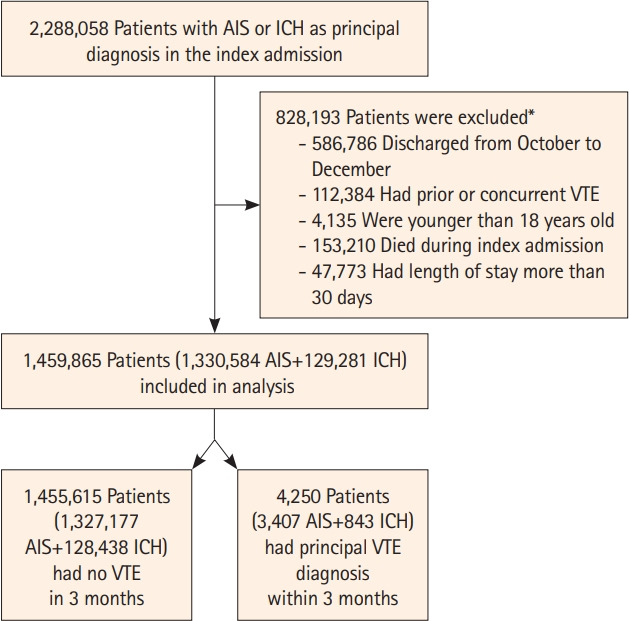
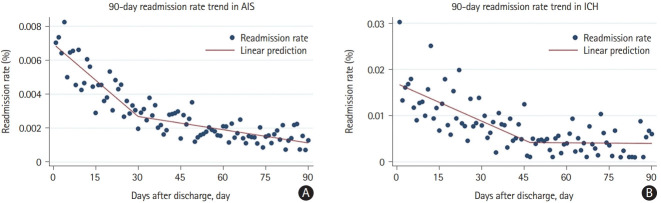
Methods: Using the Healthcare Cost and Utilization Project (HCUP) Nationwide Readmission Database, we included patients with a principal discharge diagnosis of ICH or AIS from 2016 to 2019. Patients who had VTE diagnosis or history of VTE during the index admission were excluded. We performed Cox regression models to determine factors associated with VTE readmission, compared rates between AIS and ICH and developed post-stroke VTE risk score. We estimated VTE readmission rates per day over a 90-day time window post-discharge using linear splines.
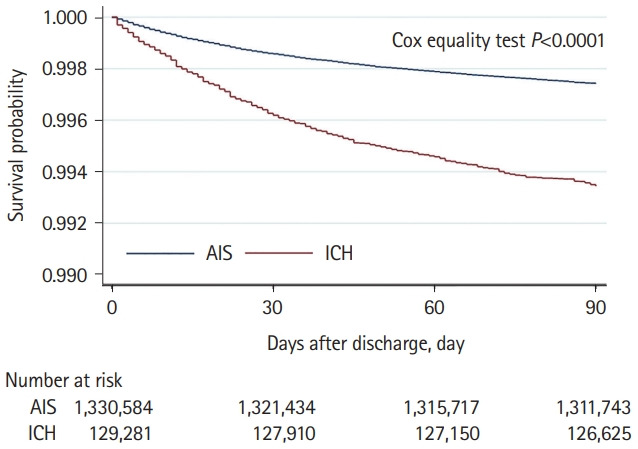
Results: Of the total 1,459,865 patients with stroke, readmission with VTE as the principal diagnosis within 90 days occurred in 0.26% (3,407/1,330,584) AIS and 0.65% (843/129,281) ICH patients. The rate of VTE readmission decreased within first 4-6 weeks (P<0.001). In AIS, cancer, obesity, higher National Institutes of Health Stroke Scale (NIHSS) score, longer hospital stay, home or rehabilitation disposition, and absence of atrial fibrillation were associated with VTE readmission. In ICH, longer hospital stay and rehabilitation disposition were associated with VTE readmission. The VTE rate was higher in ICH compared to AIS (adjusted hazard ratio 2.86, 95% confidence interval 1.93-4.25, P<0.001).
Conclusions: After stroke, VTE readmission risk is highest within the first 4-6 weeks and nearly three-fold higher after ICH vs. AIS. VTE risk is linked to decreased mobility and hypercoagulability. Studies are needed to test short-term VTE prophylaxis beyond hospitalization in high-risk patients.
Journal of StrokeCLINICAL NEUROLOGYPERIPHERAL VASCULAR DISE-PERIPHERAL VASCULAR DISEASE
CiteScore
11.00
自引率
3.70%
发文量
52
审稿时长
12 weeks
期刊介绍:
The Journal of Stroke (JoS) is a peer-reviewed publication that focuses on clinical and basic investigation of cerebral circulation and associated diseases in stroke-related fields. Its aim is to enhance patient management, education, clinical or experimental research, and professionalism. The journal covers various areas of stroke research, including pathophysiology, risk factors, symptomatology, imaging, treatment, and rehabilitation. Basic science research is included when it provides clinically relevant information. The JoS is particularly interested in studies that highlight characteristics of stroke in the Asian population, as they are underrepresented in the literature.
The JoS had an impact factor of 8.2 in 2022 and aims to provide high-quality research papers to readers while maintaining a strong reputation. It is published three times a year, on the last day of January, May, and September. The online version of the journal is considered the main version as it includes all available content. Supplementary issues are occasionally published.
The journal is indexed in various databases, including SCI(E), Pubmed, PubMed Central, Scopus, KoreaMed, Komci, Synapse, Science Central, Google Scholar, and DOI/Crossref. It is also the official journal of the Korean Stroke Society since 1999, with the abbreviated title J Stroke.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


