Kristin Colling, Alexandra K Kraft, Melissa L Harry
{"title":"Alcohol use disorder in the intensive care unit a highly morbid condition, but chemical dependency discussion improves outcomes.","authors":"Kristin Colling, Alexandra K Kraft, Melissa L Harry","doi":"10.4266/acc.2022.00584","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Alcohol use disorders (AUD) are common in patients admitted to intensive care units (ICU) and increase the risk for worse outcomes. In this study, we describe factors associated with patient mortality after ICU admission and the effect of chemical dependency (CD) counseling on outcomes in the year following ICU admission.</p><p><strong>Methods: </strong>We retrospectively reviewed patient demographics, hospital data, and documentation of CD counseling by medical providers for all ICU patients with AUD admitted to our institution between January 2017 and March 2019. Primary outcomes were in-hospital and 1-year mortality.</p><p><strong>Results: </strong>Of the 527 patients with AUD requiring ICU care, median age was 56 years (range, 18-86). Both in-hospital (12%) and 1-year mortality rates (27%) were high. Rural patients, comorbidities, older age, need for mechanical ventilation, and complications were associated with increased risk of in-hospital and 1-year mortality. CD counseling was documented for 73% of patients, and 50% of these patients accepted alcohol treatment or resources prior to discharge. CD evaluation and acceptance was associated with a significantly decreased rate of readmission for liver or alcohol-related issues (36% vs. 58%; odds ratio [OR], 0.41; 95% confidence interval [CI], 0.27-0.61) and 1-year mortality (7% vs. 19.5%; OR, 0.32; 95% CI, 0.16-0.64). CD evaluation alone, regardless of patient acceptance, was associated with a significantly decreased 1-year post-discharge mortality rate (12% vs. 23%; OR, 0.44; 95% CI, 0.25-0.77).</p><p><strong>Conclusions: </strong>ICU patients with AUD had high in-hospital and 1-year mortality. CD evaluation, regardless of patient acceptance, was associated with a significant decrease in 1-year mortality.</p>","PeriodicalId":44118,"journal":{"name":"Acute and Critical Care","volume":null,"pages":null},"PeriodicalIF":1.7000,"publicationDate":"2023-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/fb/1f/acc-2022-00584.PMC10030241.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute and Critical Care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4266/acc.2022.00584","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/10 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Alcohol use disorders (AUD) are common in patients admitted to intensive care units (ICU) and increase the risk for worse outcomes. In this study, we describe factors associated with patient mortality after ICU admission and the effect of chemical dependency (CD) counseling on outcomes in the year following ICU admission.
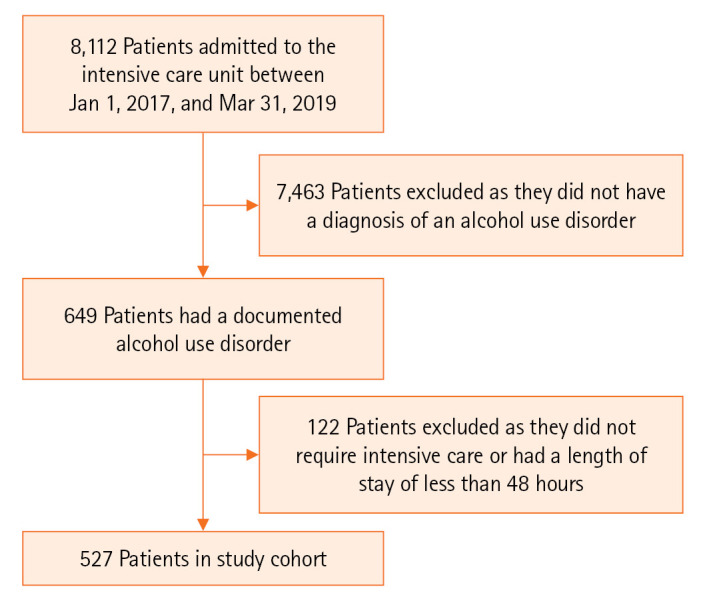
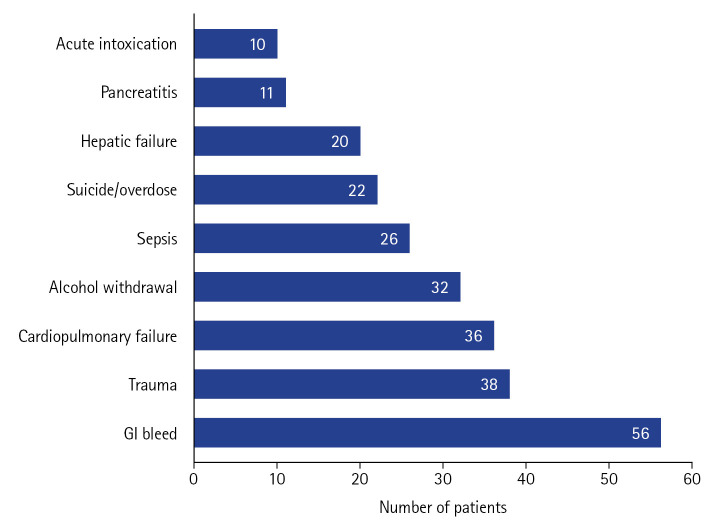
Methods: We retrospectively reviewed patient demographics, hospital data, and documentation of CD counseling by medical providers for all ICU patients with AUD admitted to our institution between January 2017 and March 2019. Primary outcomes were in-hospital and 1-year mortality.
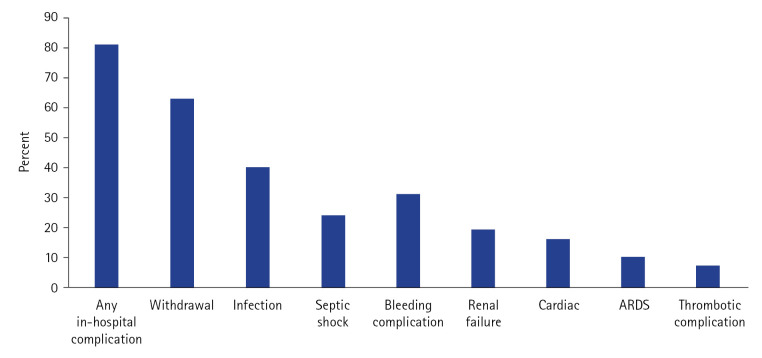
Results: Of the 527 patients with AUD requiring ICU care, median age was 56 years (range, 18-86). Both in-hospital (12%) and 1-year mortality rates (27%) were high. Rural patients, comorbidities, older age, need for mechanical ventilation, and complications were associated with increased risk of in-hospital and 1-year mortality. CD counseling was documented for 73% of patients, and 50% of these patients accepted alcohol treatment or resources prior to discharge. CD evaluation and acceptance was associated with a significantly decreased rate of readmission for liver or alcohol-related issues (36% vs. 58%; odds ratio [OR], 0.41; 95% confidence interval [CI], 0.27-0.61) and 1-year mortality (7% vs. 19.5%; OR, 0.32; 95% CI, 0.16-0.64). CD evaluation alone, regardless of patient acceptance, was associated with a significantly decreased 1-year post-discharge mortality rate (12% vs. 23%; OR, 0.44; 95% CI, 0.25-0.77).
Conclusions: ICU patients with AUD had high in-hospital and 1-year mortality. CD evaluation, regardless of patient acceptance, was associated with a significant decrease in 1-year mortality.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


