Kangho Lee, Dongyeon Ryu, Hohyun Kim, Sungjin Park, Sangbong Lee, Chanik Park, Gilhwan Kim, Sunhyun Kim, Nahyeon Lee
{"title":"Selection of appropriate reference creatinine estimate for acute kidney injury diagnosis in patients with severe trauma.","authors":"Kangho Lee, Dongyeon Ryu, Hohyun Kim, Sungjin Park, Sangbong Lee, Chanik Park, Gilhwan Kim, Sunhyun Kim, Nahyeon Lee","doi":"10.4266/acc.2022.01046","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In patients with severe trauma, the diagnosis of acute kidney injury (AKI) is important because it is a predictive factor for poor prognosis and can affect patient care. The diagnosis and staging of AKI are based on change in serum creatinine (SCr) levels from baseline. However, baseline creatinine levels in patients with traumatic injuries are often unknown, making the diagnosis of AKI in trauma patients difficult. This study aimed to enhance the accuracy of AKI diagnosis in trauma patients by presenting an appropriate reference creatinine estimate (RCE).</p><p><strong>Methods: </strong>We reviewed adult patients with severe trauma requiring intensive care unit admission between 2015 and 2019 (n=3,228) at a single regional trauma center in South Korea. AKI was diagnosed based on the current guideline published by the Kidney Disease: Improving Global Outcomes organization. AKI was determined using the following RCEs: estimated SCr75-modification of diet in renal disease (MDRD), trauma MDRD (TMDRD), admission creatinine level, and first-day creatinine nadir. We assessed inclusivity, prognostic ability, and incrementality using the different RCEs.</p><p><strong>Results: </strong>The incidence of AKI varied from 15% to 46% according to the RCE used. The receiver operating characteristic curve of TMDRD used to predict mortality and the need for renal replacement therapy (RRT) had the highest value and was statistically significant (0.797, P<0.001; 0.890, P=0.002, respectively). In addition, the use of TMDRD resulted in a mortality prognostic ability and the need for RRT was incremental with AKI stage.</p><p><strong>Conclusions: </strong>In this study, TMDRD was feasible as a RCE, resulting in optimal post-traumatic AKI diagnosis and prognosis.</p>","PeriodicalId":44118,"journal":{"name":"Acute and Critical Care","volume":null,"pages":null},"PeriodicalIF":1.7000,"publicationDate":"2023-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/db/74/acc-2022-01046.PMC10030240.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute and Critical Care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4266/acc.2022.01046","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In patients with severe trauma, the diagnosis of acute kidney injury (AKI) is important because it is a predictive factor for poor prognosis and can affect patient care. The diagnosis and staging of AKI are based on change in serum creatinine (SCr) levels from baseline. However, baseline creatinine levels in patients with traumatic injuries are often unknown, making the diagnosis of AKI in trauma patients difficult. This study aimed to enhance the accuracy of AKI diagnosis in trauma patients by presenting an appropriate reference creatinine estimate (RCE).
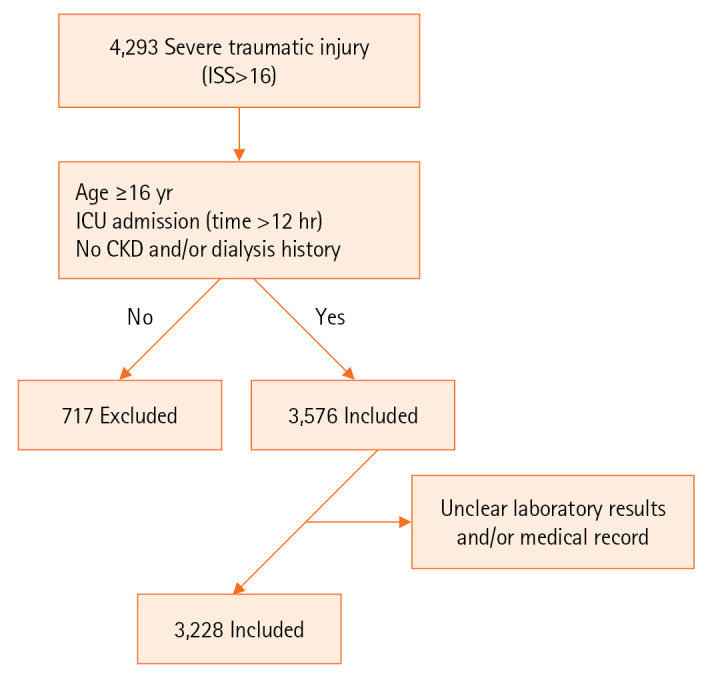
Methods: We reviewed adult patients with severe trauma requiring intensive care unit admission between 2015 and 2019 (n=3,228) at a single regional trauma center in South Korea. AKI was diagnosed based on the current guideline published by the Kidney Disease: Improving Global Outcomes organization. AKI was determined using the following RCEs: estimated SCr75-modification of diet in renal disease (MDRD), trauma MDRD (TMDRD), admission creatinine level, and first-day creatinine nadir. We assessed inclusivity, prognostic ability, and incrementality using the different RCEs.
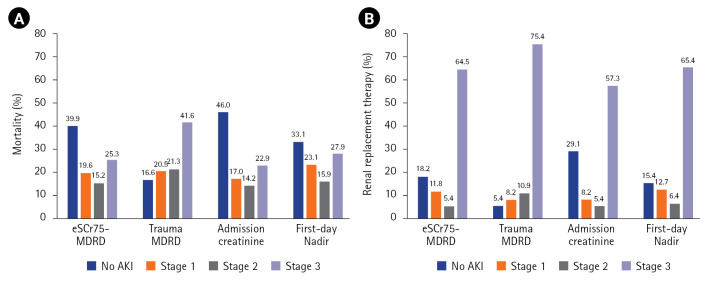
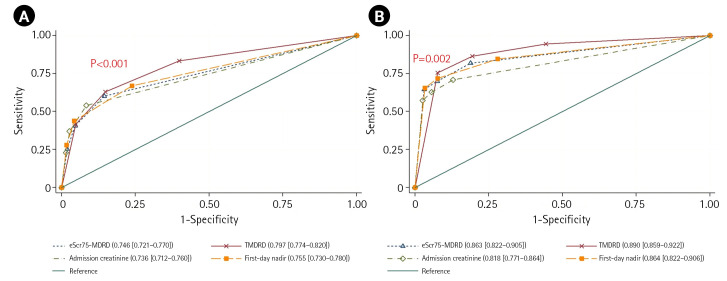
Results: The incidence of AKI varied from 15% to 46% according to the RCE used. The receiver operating characteristic curve of TMDRD used to predict mortality and the need for renal replacement therapy (RRT) had the highest value and was statistically significant (0.797, P<0.001; 0.890, P=0.002, respectively). In addition, the use of TMDRD resulted in a mortality prognostic ability and the need for RRT was incremental with AKI stage.
Conclusions: In this study, TMDRD was feasible as a RCE, resulting in optimal post-traumatic AKI diagnosis and prognosis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


