Inter-observer and intra-observer variability in ultrasound assessment of gastric content and volume in critically ill patients receiving enteral nutrition.
{"title":"Inter-observer and intra-observer variability in ultrasound assessment of gastric content and volume in critically ill patients receiving enteral nutrition.","authors":"Héctor Andrés Ruiz Ávila, Carmelo José Espinosa Almanza, Cindy Yohana Fuentes Barreiro","doi":"10.1186/s13089-023-00312-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The assessment of gastric content and volume using bedside ultrasound (US) has become a useful tool in emergency departments, anesthesiology departments and inpatient wards, as it provides a rapid and dynamic assessment of the gastric content of patients, which, allows making decisions regarding the risk of regurgitation or the need to adjust the strategy used to induce general anesthesia in patients with a full stomach. This assessment consists of two evaluations: a qualitative one, in which the status of the antrum, in terms of gastric content, is classified into three categories (empty, liquid content and full), and a quantitative one, where gastric volume is estimated. The objective of this study was to estimate the intra-observer and inter-observer agreement in ultrasound assessment of gastric content and volume in critically ill patients receiving enteral nutrition.</p><p><strong>Results: </strong>A total of 41 patients were included and each examiner performed 64 gastric US (n = 128). Participants' average age was 56.5 years (SD ± 12.6) and 63.4% were men. Regarding the qualitative evaluation of the antrum, in supine position both examiners classified the gastric content as grade 0 in 1 gastric US (1.5%), grade 1 in 4 gastric US (6.2%) and grade 2 in 59 (92.1%). Regarding intra-observer variability in the measurement of the area of the antrum, Lin's concordance correlation coefficient (CCC), the difference of means between measurements and the 95% limits of agreement of Bland and Altman values were 0.95 (95% CI 0.940-0.977), - 0.47 cm<sup>2</sup> (SD ± 1.64) and - 3.70 cm<sup>2</sup> to 2.75 cm<sup>2</sup>, respectively, in EC1, and 0.94 (95% CI 0.922-0.973), - 0.18 cm<sup>2</sup> (SD ± 2.18) and - 4.47 cm<sup>2</sup> to 4.09 cm<sup>2</sup> in EC2. Concerning to inter-observer variability (EC1 vs EC2) in the measurement of the area of the antrum and of gastric volume, the following CCC, mean difference between measurements and 95% limits of agreement of Bland and Altman values were obtained: measurement of the area of the antrum: 0.84 (95% CI 0.778-0.911), - 0.86 cm<sup>2</sup> (SD ± 3.38) and - 7.50 cm<sup>2</sup> to 5.78 cm<sup>2</sup>; gastric volume measurement: 0.84 (95% CI 0.782-0.913), - 12.3 mL (SD ± 49.2) and - 108.8 mL to 84.0 mL.</p><p><strong>Conclusions: </strong>The assessment of gastric content and volume using bedside US in critically ill patients on mechanical ventilation and receiving enteral nutrition showed a good intra and inter-rater reliability. Most of the patients included in the study had a high risk of pulmonary aspiration, since, according to the results of the gastric US evaluation, they had gastric volumes > 1.5 mL/kg.</p>","PeriodicalId":75201,"journal":{"name":"","volume":"15 1","pages":"14"},"PeriodicalIF":0.0,"publicationDate":"2023-03-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10024819/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-023-00312-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The assessment of gastric content and volume using bedside ultrasound (US) has become a useful tool in emergency departments, anesthesiology departments and inpatient wards, as it provides a rapid and dynamic assessment of the gastric content of patients, which, allows making decisions regarding the risk of regurgitation or the need to adjust the strategy used to induce general anesthesia in patients with a full stomach. This assessment consists of two evaluations: a qualitative one, in which the status of the antrum, in terms of gastric content, is classified into three categories (empty, liquid content and full), and a quantitative one, where gastric volume is estimated. The objective of this study was to estimate the intra-observer and inter-observer agreement in ultrasound assessment of gastric content and volume in critically ill patients receiving enteral nutrition.
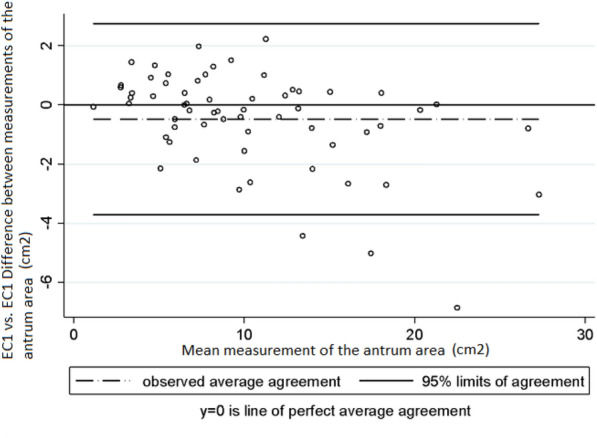
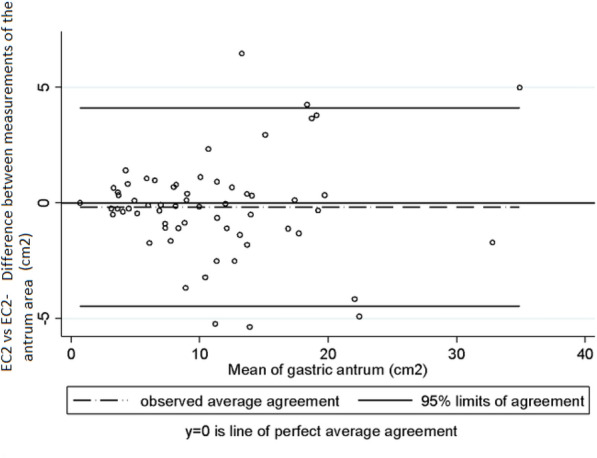
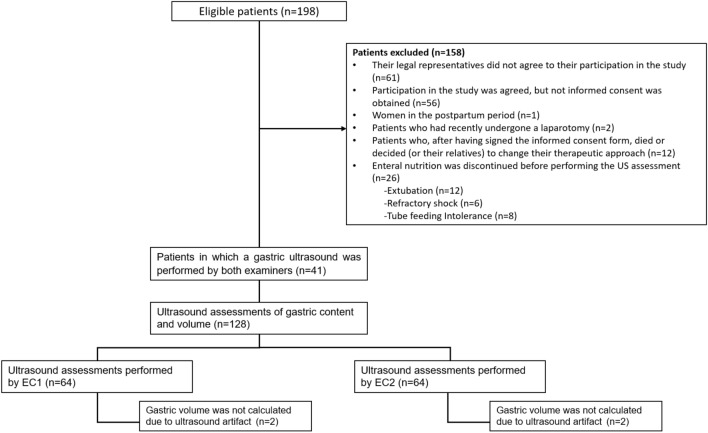
Results: A total of 41 patients were included and each examiner performed 64 gastric US (n = 128). Participants' average age was 56.5 years (SD ± 12.6) and 63.4% were men. Regarding the qualitative evaluation of the antrum, in supine position both examiners classified the gastric content as grade 0 in 1 gastric US (1.5%), grade 1 in 4 gastric US (6.2%) and grade 2 in 59 (92.1%). Regarding intra-observer variability in the measurement of the area of the antrum, Lin's concordance correlation coefficient (CCC), the difference of means between measurements and the 95% limits of agreement of Bland and Altman values were 0.95 (95% CI 0.940-0.977), - 0.47 cm2 (SD ± 1.64) and - 3.70 cm2 to 2.75 cm2, respectively, in EC1, and 0.94 (95% CI 0.922-0.973), - 0.18 cm2 (SD ± 2.18) and - 4.47 cm2 to 4.09 cm2 in EC2. Concerning to inter-observer variability (EC1 vs EC2) in the measurement of the area of the antrum and of gastric volume, the following CCC, mean difference between measurements and 95% limits of agreement of Bland and Altman values were obtained: measurement of the area of the antrum: 0.84 (95% CI 0.778-0.911), - 0.86 cm2 (SD ± 3.38) and - 7.50 cm2 to 5.78 cm2; gastric volume measurement: 0.84 (95% CI 0.782-0.913), - 12.3 mL (SD ± 49.2) and - 108.8 mL to 84.0 mL.
Conclusions: The assessment of gastric content and volume using bedside US in critically ill patients on mechanical ventilation and receiving enteral nutrition showed a good intra and inter-rater reliability. Most of the patients included in the study had a high risk of pulmonary aspiration, since, according to the results of the gastric US evaluation, they had gastric volumes > 1.5 mL/kg.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


