{"title":"Pyopericardium and extensive mediastinal abscess following EBUS-TBNA for mediastinal staging of NSCLC: a case report.","authors":"Marc Hartert, Michael Wolf, Martin Huertgen","doi":"10.21037/med-22-13","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Based on the algorithm on preoperative mediastinal staging in patients with non-small cell lung cancer (NSCLC), endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) is indicated in case of computed tomography (CT)-enlarged or positron emission tomography (PET)-positive mediastinal lymph nodes. It represents both a safe minimal invasive procedure with complication rates of less than 1.5% and a valid tool with a high sensitivity defining mediastinal nodal disease. However, infectious complications like mediastinitis or pyopericardium are most feared.</p><p><strong>Case description: </strong>A 54-year-old woman was admitted to our hospital for further investigation of a suspected NSCLC of the right upper lobe. EBUS-TBNA was performed to receive both diagnosis and samples of the mediastinal lymph nodes. Two weeks after EBUS-TBNA, the patient presented with symptoms of cardiogenic/septic shock: hypotension, tachycardia, chest pain and fever. Prompt diagnosis of concomitant infectious mediastinitis and extensive pyopericardium in consequence of EBUS-TBNA was obvious. Besides systemic antibiotics, bilateral thoracoscopic interventions finally made the breakthrough. The patient could be discharged roughly three weeks after emergent re-admittance. As being finally diagnosed with NSCLC (stage IIIA squamous cell carcinoma), the patient underwent-subsequent to induction chemotherapy-a definitive sequential chemoradiotherapy. Twelve-month follow-up confirmed stable disease.</p><p><strong>Conclusions: </strong>It is to be expected that with increasing application of EBUS-TBNA as mediastinal staging tool, the number of serious infection-related complications will rise accordingly. The efficacy of antibiotic prophylaxis after EBUS-TBNA has not yet been proved and is therefore not included in any guideline. Our case gives an impression on the severity of delayed infectious complications after EBUS-TBNA and outlines up-front surgery as primary objective to broadly debride all contagious abscess-/empyema sites. With increased use of EBUS-TBNA as mediastinal staging tool, clinicians should be aware of this rare but highly critical peri-interventional complication in order to closely monitor endangered patients.</p>","PeriodicalId":74139,"journal":{"name":"Mediastinum (Hong Kong, China)","volume":"7 ","pages":"4"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d3/48/med-07-4.PMC10011863.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mediastinum (Hong Kong, China)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/med-22-13","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Based on the algorithm on preoperative mediastinal staging in patients with non-small cell lung cancer (NSCLC), endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) is indicated in case of computed tomography (CT)-enlarged or positron emission tomography (PET)-positive mediastinal lymph nodes. It represents both a safe minimal invasive procedure with complication rates of less than 1.5% and a valid tool with a high sensitivity defining mediastinal nodal disease. However, infectious complications like mediastinitis or pyopericardium are most feared.
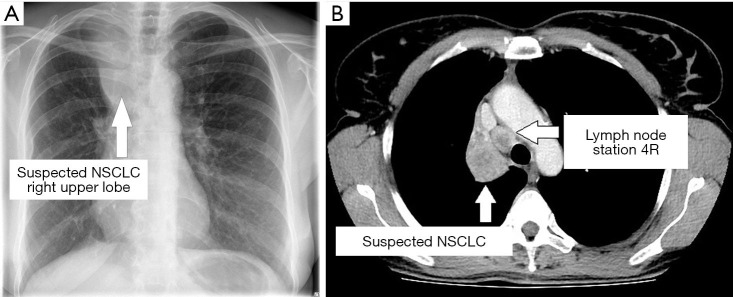
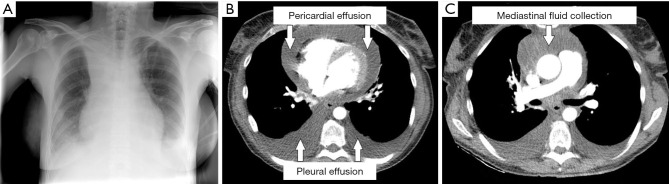
Case description: A 54-year-old woman was admitted to our hospital for further investigation of a suspected NSCLC of the right upper lobe. EBUS-TBNA was performed to receive both diagnosis and samples of the mediastinal lymph nodes. Two weeks after EBUS-TBNA, the patient presented with symptoms of cardiogenic/septic shock: hypotension, tachycardia, chest pain and fever. Prompt diagnosis of concomitant infectious mediastinitis and extensive pyopericardium in consequence of EBUS-TBNA was obvious. Besides systemic antibiotics, bilateral thoracoscopic interventions finally made the breakthrough. The patient could be discharged roughly three weeks after emergent re-admittance. As being finally diagnosed with NSCLC (stage IIIA squamous cell carcinoma), the patient underwent-subsequent to induction chemotherapy-a definitive sequential chemoradiotherapy. Twelve-month follow-up confirmed stable disease.
Conclusions: It is to be expected that with increasing application of EBUS-TBNA as mediastinal staging tool, the number of serious infection-related complications will rise accordingly. The efficacy of antibiotic prophylaxis after EBUS-TBNA has not yet been proved and is therefore not included in any guideline. Our case gives an impression on the severity of delayed infectious complications after EBUS-TBNA and outlines up-front surgery as primary objective to broadly debride all contagious abscess-/empyema sites. With increased use of EBUS-TBNA as mediastinal staging tool, clinicians should be aware of this rare but highly critical peri-interventional complication in order to closely monitor endangered patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


