Subcutaneous Versus Transvenous Implantable Defibrillator Therapy: A Systematic Review and Meta-Analysis of Randomized Trials and Propensity Score-Matched Studies.
Khi Yung Fong, Colin Jun Rong Ng, Yue Wang, Colin Yeo, Vern Hsen Tan
{"title":"Subcutaneous Versus Transvenous Implantable Defibrillator Therapy: A Systematic Review and Meta-Analysis of Randomized Trials and Propensity Score-Matched Studies.","authors":"Khi Yung Fong, Colin Jun Rong Ng, Yue Wang, Colin Yeo, Vern Hsen Tan","doi":"10.1161/JAHA.121.024756","DOIUrl":null,"url":null,"abstract":"<p><p>Background Subcutaneous implantable cardioverter-defibrillators (S-ICDs) have been of great interest as an alternative to transvenous implantable cardioverter-defibrillators (TV-ICDs). No meta-analyses synthesizing data from high-quality studies have yet been published. Methods and Results An electronic literature search was conducted to retrieve randomized controlled trials or propensity score-matched studies comparing S-ICD against TV-ICD in patients with an implantable cardioverter-defibrillator indication. The primary outcomes were device-related complications and lead-related complications. Secondary outcomes were inappropriate shocks, appropriate shock, all-cause mortality, and infection. All outcomes were pooled under random-effects meta-analyses and reported as risk ratios (RRs) and 95% CIs. Kaplan-Meier curves of device-related complications were digitized to retrieve individual patient data and pooled under a 1-stage meta-analysis using Cox models to determine hazard ratios (HRs) of patients undergoing S-ICD versus TV-ICD. A total of 5 studies (2387 patients) were retrieved. S-ICD had a similar rate of device-related complications compared with TV-ICD (RR, 0.59 [95% CI, 0.33-1.04]; <i>P</i>=0.070), but a significantly lower lead-related complication rate (RR, 0.14 [95% CI, 0.07-0.29]; <i>P</i><0.0001). The individual patient data-based 1-stage stratified Cox model for device-related complications across 4 studies yielded no significant difference (shared-frailty HR, 0.82 [95% CI, 0.61-1.09]; <i>P</i>=0.167), but visual inspection of pooled Kaplan-Meier curves suggested a divergence favoring S-ICD. Secondary outcomes did not differ significantly between both modalities. Conclusions S-ICD is clinically superior to TV-ICD in terms of lead-related complications while demonstrating comparable efficacy and safety. For device-related complications, S-ICD may be beneficial over TV-ICD in the long term. These indicate that S-ICD is likely a suitable substitute for TV-ICD in patients requiring implantable cardioverter-defibrillator implantation without a pacing indication.</p>","PeriodicalId":17189,"journal":{"name":"Journal of the American Heart Association: Cardiovascular and Cerebrovascular Disease","volume":"94 1","pages":"e024756"},"PeriodicalIF":0.0000,"publicationDate":"2022-06-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9238723/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American Heart Association: Cardiovascular and Cerebrovascular Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1161/JAHA.121.024756","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/6/3 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
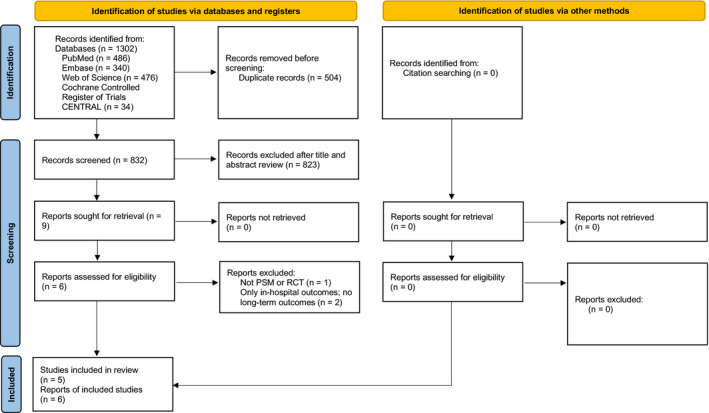
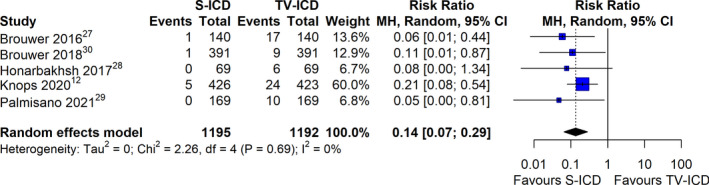
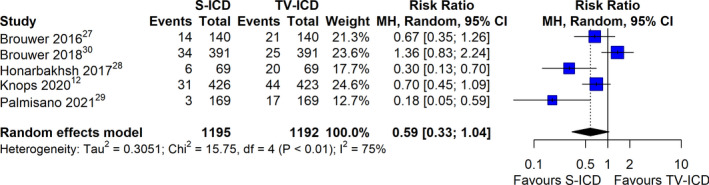
Background Subcutaneous implantable cardioverter-defibrillators (S-ICDs) have been of great interest as an alternative to transvenous implantable cardioverter-defibrillators (TV-ICDs). No meta-analyses synthesizing data from high-quality studies have yet been published. Methods and Results An electronic literature search was conducted to retrieve randomized controlled trials or propensity score-matched studies comparing S-ICD against TV-ICD in patients with an implantable cardioverter-defibrillator indication. The primary outcomes were device-related complications and lead-related complications. Secondary outcomes were inappropriate shocks, appropriate shock, all-cause mortality, and infection. All outcomes were pooled under random-effects meta-analyses and reported as risk ratios (RRs) and 95% CIs. Kaplan-Meier curves of device-related complications were digitized to retrieve individual patient data and pooled under a 1-stage meta-analysis using Cox models to determine hazard ratios (HRs) of patients undergoing S-ICD versus TV-ICD. A total of 5 studies (2387 patients) were retrieved. S-ICD had a similar rate of device-related complications compared with TV-ICD (RR, 0.59 [95% CI, 0.33-1.04]; P=0.070), but a significantly lower lead-related complication rate (RR, 0.14 [95% CI, 0.07-0.29]; P<0.0001). The individual patient data-based 1-stage stratified Cox model for device-related complications across 4 studies yielded no significant difference (shared-frailty HR, 0.82 [95% CI, 0.61-1.09]; P=0.167), but visual inspection of pooled Kaplan-Meier curves suggested a divergence favoring S-ICD. Secondary outcomes did not differ significantly between both modalities. Conclusions S-ICD is clinically superior to TV-ICD in terms of lead-related complications while demonstrating comparable efficacy and safety. For device-related complications, S-ICD may be beneficial over TV-ICD in the long term. These indicate that S-ICD is likely a suitable substitute for TV-ICD in patients requiring implantable cardioverter-defibrillator implantation without a pacing indication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


