Interim Report of a Japanese Phase II Trial for Cardiac Stereotactic Body Radiotherapy in Refractory Ventricular Tachycardia - Focus on Target Determination.
{"title":"Interim Report of a Japanese Phase II Trial for Cardiac Stereotactic Body Radiotherapy in Refractory Ventricular Tachycardia - Focus on Target Determination.","authors":"Mari Amino, Shigeto Kabuki, Etsuo Kunieda, Jun Hashimoto, Akitomo Sugawara, Tetsuri Sakai, Susumu Sakama, Kengo Ayabe, Yohei Ohno, Atsuhiko Yagishita, Yoshinori Kobayashi, Yuji Ikari, Koichiro Yoshioka","doi":"10.1253/circrep.CR-23-0003","DOIUrl":null,"url":null,"abstract":"<p><p><b><i>Background:</i></b> Cardiac radiotherapy using stereotactic body radiation therapy (SBRT) has attracted attention as a minimally invasive treatment for refractory ventricular tachycardia. However, a standardized protocol and software program for determining the irradiation target have not been established. Here, we report the first preclinical stereotactic radioregulation antiarrhythmic therapy trial in Japan, focused on the target-setting process. <b><i>Methods and Results:</i></b> From 2019 onwards, 3 patients (age range 60-91 years) presenting with ischemic or non-ischemic cardiomyopathy were enrolled. Two patients were extremely serious and urgent, and were followed up for 6 and 30 months. To determine the irradiation targets, we aggregated electrophysiological, structural, and functional data and reflected them in an American Heart Association 17-segment model, as per the current recommendations. However, in all 3 patients, invasive electrophysiological study, phase-contrast computed tomography, and magnetic resonance imaging could not be performed; therefore, electrophysiological and structural information was limited. As alternatives, high-resolution ambulatory electrocardiography and nuclear medicine studies were useful in assessing arrhythmic substrates; however, concerns regarding test weighting and multiple scoring remain. Risks to surrounding organs were fully taken into account. <b><i>Conclusions:</i></b> In patients requiring cardiac SBRT, the information needed for target planning is sometimes limited to minimally invasive tests. Although there are issues to be resolved, this is a promising option for the life-saving treatment of patients in critical situations.</p>","PeriodicalId":10276,"journal":{"name":"Circulation Reports","volume":"5 3","pages":"69-79"},"PeriodicalIF":0.0000,"publicationDate":"2023-03-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/fb/6e/circrep-5-69.PMC9992511.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Circulation Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1253/circrep.CR-23-0003","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
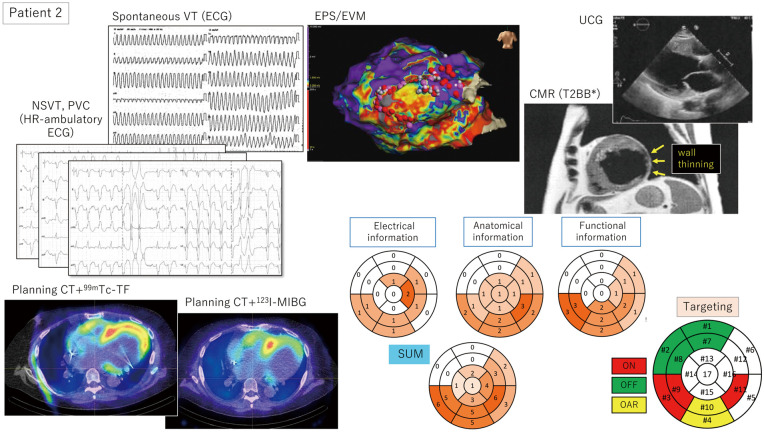
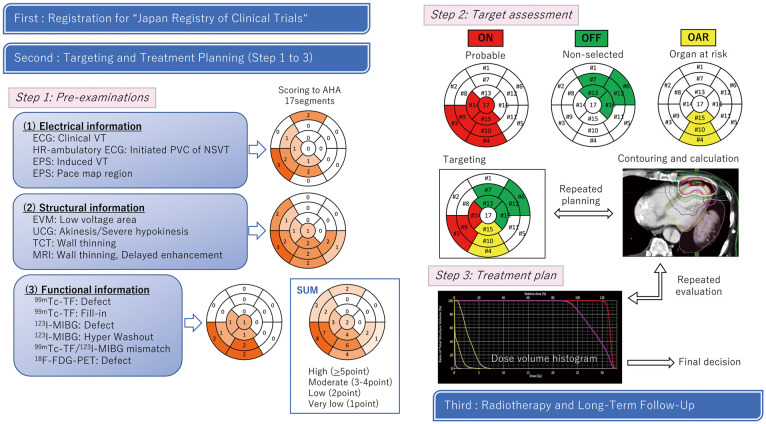
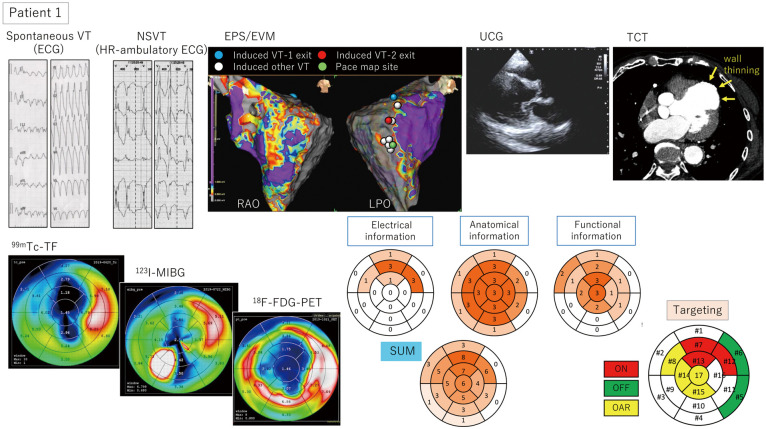
Background: Cardiac radiotherapy using stereotactic body radiation therapy (SBRT) has attracted attention as a minimally invasive treatment for refractory ventricular tachycardia. However, a standardized protocol and software program for determining the irradiation target have not been established. Here, we report the first preclinical stereotactic radioregulation antiarrhythmic therapy trial in Japan, focused on the target-setting process. Methods and Results: From 2019 onwards, 3 patients (age range 60-91 years) presenting with ischemic or non-ischemic cardiomyopathy were enrolled. Two patients were extremely serious and urgent, and were followed up for 6 and 30 months. To determine the irradiation targets, we aggregated electrophysiological, structural, and functional data and reflected them in an American Heart Association 17-segment model, as per the current recommendations. However, in all 3 patients, invasive electrophysiological study, phase-contrast computed tomography, and magnetic resonance imaging could not be performed; therefore, electrophysiological and structural information was limited. As alternatives, high-resolution ambulatory electrocardiography and nuclear medicine studies were useful in assessing arrhythmic substrates; however, concerns regarding test weighting and multiple scoring remain. Risks to surrounding organs were fully taken into account. Conclusions: In patients requiring cardiac SBRT, the information needed for target planning is sometimes limited to minimally invasive tests. Although there are issues to be resolved, this is a promising option for the life-saving treatment of patients in critical situations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


