A comparison of perinatal outcomes following fresh blastocyst or cleavage stage embryo transfer in singletons and twins and between singleton siblings.
Edwin-Amalraj Raja, Siladitya Bhattacharya, Abha Maheshwari, David J McLernon
{"title":"A comparison of perinatal outcomes following fresh blastocyst or cleavage stage embryo transfer in singletons and twins and between singleton siblings.","authors":"Edwin-Amalraj Raja, Siladitya Bhattacharya, Abha Maheshwari, David J McLernon","doi":"10.1093/hropen/hoad003","DOIUrl":null,"url":null,"abstract":"<p><strong>Study question: </strong>Are perinatal outcomes following fresh blastocyst versus fresh cleavage stage embryo transfer (ET) different in singletons, twins, and between singleton siblings?</p><p><strong>Summary answer: </strong>Singleton babies conceived following fresh blastocyst, versus cleavage stage, ET are less likely to be small for gestational age (SGA) or to have a congenital anomaly (a result confirmed by comparing singleton siblings), while singletons born following fresh blastocyst ET were at a higher risk of being large for gestational age (LGA) than their sibling born following fresh cleavage stage ET.</p><p><strong>What is known already: </strong>Blastocyst stage transfer is now the preferred strategy in most IVF units. Previous studies have suggested that babies conceived through blastocyst transfer are at increased risk of preterm birth and LGA.</p><p><strong>Study design size duration: </strong>A national population-based retrospective cohort study was performed using linked Human Fertilisation and Embryology Authority (HFEA) data on 130 516 IVF and ICSI livebirths occurring from 103 062 women between 2000 and 2017.</p><p><strong>Participants/materials setting methods: </strong>We included women who had at least one singleton livebirth resulting from IVF/ICSI fresh embryo treatment, using their own eggs and partner's sperm. A linked HFEA dataset was analysed using a multilevel framework, which accommodated repeated IVF cycles resulting in livebirths in the same woman. A population-averaged robust Poisson model was used for binary outcomes and a multinomial logistic regression model was used for categorical outcomes. Unadjusted and adjusted risk ratios (aRRs) (95% CI) were calculated.</p><p><strong>Main results and the role of chance: </strong>There were 130 516 livebirths in 103 062 women, including 86 630 singletons, 43 886 twin births, and 5384 pairs of singleton siblings. In comparison with fresh cleavage stage ET, fresh blastocyst stage transfer in singletons was associated with a lower risk of low birthweight (aRR = 0.92; 95% CI 0.86, 0.99), lower risk of being SGA (0.83; 0.78, 0.89), and lower risk of congenital anomaly (0.79; 0.71, 0.89). This analysis did not show an increase in risk associated with preterm birth (1.00; 0.94, 1.06), high birthweight (0.99; 0.93, 1.06), LGA (0.99; 0.93, 1.05), and the chance of healthy singleton baby (1.00; 1.00, 1.02). Twins resulting from fresh blastocyst stage ET were at slightly higher risk of preterm birth (1.05; 1.02, 1.10) compared with twins conceived following fresh cleavage stage ET. There was insufficient evidence for an association with the other perinatal outcomes. Singleton siblings born following fresh blastocyst stage ET were at a higher risk of being LGA (1.57; 1.01, 2.46) and at lower risk of having a congenital anomaly (0.52; 0.28, 0.97) compared to their singleton siblings born following cleavage stage ET. There was some evidence of excess risk of preterm birth (1.42; 0.97, 2.23) associated with blastocyst stage transfer. However, we could not confirm an association between blastocyst stage ET and low birthweight (1.35; 0.81, 2.27), high birthweight (1.19; 0.80, 1.77), and the chance of being a healthy baby (0.97; 0.86, 1.09).</p><p><strong>Limitations reasons for caution: </strong>This was an observational study where we were unable to adjust for some key confounders, such as maternal smoking status and BMI, which may change from one pregnancy to another and are not recorded in the HFEA dataset.</p><p><strong>Wider implications of the findings: </strong>In the largest study of its kind, our analysis of singleton siblings, corrected for unmeasured, non-time varying maternal factors, confirms the previously reported association between blastocyst transfer and LGA babies, and shows a reduced risk of congenital anomaly following blastocyst transfer. Our sibling analysis did not confirm a decreased risk of low birthweight following blastocyst transfer. Overall, absolute risks are low and there is insufficient evidence to challenge the practice of extended culture of embryos.</p><p><strong>Study funding/competing interests: </strong>This project is financed by an NHS Grampian Endowment Research Grant, project number 17/052. One of the authors, S.B., was the Editor in Chief of <i>HROpen</i> until 31 December 2022 and would have been in that role when the paper was first submitted. As an invited speaker, S.B. has received travel expenses, accommodation and honoraria from Merck, Organon, and Ferring. A.M. has received travel expenses, accommodation, and honoraria from Merck Serono, Cook Medical, Pharmasure, Gedeon Richter, and Ferring. D.J.M. is currently a <i>HROpen</i> Associate Editor.</p><p><strong>Trial registration number: </strong>N/A.</p>","PeriodicalId":73264,"journal":{"name":"Human reproduction open","volume":"2023 2","pages":"hoad003"},"PeriodicalIF":8.3000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9995092/pdf/","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Human reproduction open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/hropen/hoad003","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 2
Abstract
Study question: Are perinatal outcomes following fresh blastocyst versus fresh cleavage stage embryo transfer (ET) different in singletons, twins, and between singleton siblings?
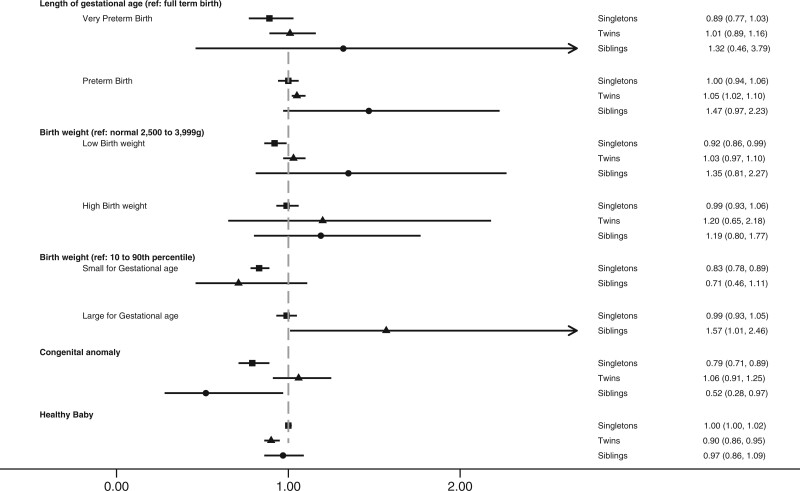
Summary answer: Singleton babies conceived following fresh blastocyst, versus cleavage stage, ET are less likely to be small for gestational age (SGA) or to have a congenital anomaly (a result confirmed by comparing singleton siblings), while singletons born following fresh blastocyst ET were at a higher risk of being large for gestational age (LGA) than their sibling born following fresh cleavage stage ET.
What is known already: Blastocyst stage transfer is now the preferred strategy in most IVF units. Previous studies have suggested that babies conceived through blastocyst transfer are at increased risk of preterm birth and LGA.
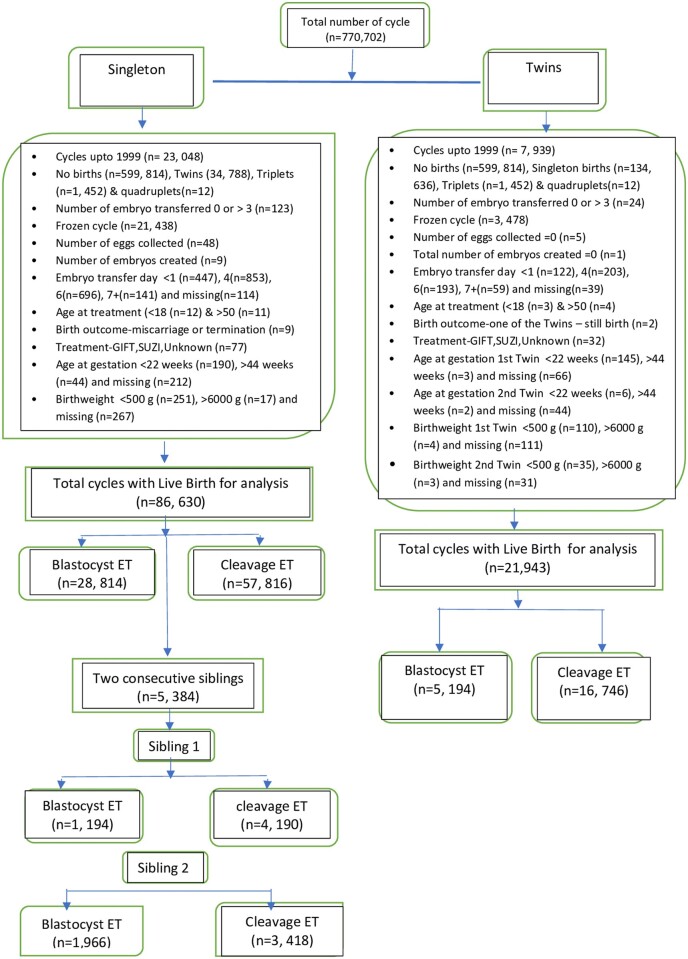
Study design size duration: A national population-based retrospective cohort study was performed using linked Human Fertilisation and Embryology Authority (HFEA) data on 130 516 IVF and ICSI livebirths occurring from 103 062 women between 2000 and 2017.
Participants/materials setting methods: We included women who had at least one singleton livebirth resulting from IVF/ICSI fresh embryo treatment, using their own eggs and partner's sperm. A linked HFEA dataset was analysed using a multilevel framework, which accommodated repeated IVF cycles resulting in livebirths in the same woman. A population-averaged robust Poisson model was used for binary outcomes and a multinomial logistic regression model was used for categorical outcomes. Unadjusted and adjusted risk ratios (aRRs) (95% CI) were calculated.
Main results and the role of chance: There were 130 516 livebirths in 103 062 women, including 86 630 singletons, 43 886 twin births, and 5384 pairs of singleton siblings. In comparison with fresh cleavage stage ET, fresh blastocyst stage transfer in singletons was associated with a lower risk of low birthweight (aRR = 0.92; 95% CI 0.86, 0.99), lower risk of being SGA (0.83; 0.78, 0.89), and lower risk of congenital anomaly (0.79; 0.71, 0.89). This analysis did not show an increase in risk associated with preterm birth (1.00; 0.94, 1.06), high birthweight (0.99; 0.93, 1.06), LGA (0.99; 0.93, 1.05), and the chance of healthy singleton baby (1.00; 1.00, 1.02). Twins resulting from fresh blastocyst stage ET were at slightly higher risk of preterm birth (1.05; 1.02, 1.10) compared with twins conceived following fresh cleavage stage ET. There was insufficient evidence for an association with the other perinatal outcomes. Singleton siblings born following fresh blastocyst stage ET were at a higher risk of being LGA (1.57; 1.01, 2.46) and at lower risk of having a congenital anomaly (0.52; 0.28, 0.97) compared to their singleton siblings born following cleavage stage ET. There was some evidence of excess risk of preterm birth (1.42; 0.97, 2.23) associated with blastocyst stage transfer. However, we could not confirm an association between blastocyst stage ET and low birthweight (1.35; 0.81, 2.27), high birthweight (1.19; 0.80, 1.77), and the chance of being a healthy baby (0.97; 0.86, 1.09).
Limitations reasons for caution: This was an observational study where we were unable to adjust for some key confounders, such as maternal smoking status and BMI, which may change from one pregnancy to another and are not recorded in the HFEA dataset.
Wider implications of the findings: In the largest study of its kind, our analysis of singleton siblings, corrected for unmeasured, non-time varying maternal factors, confirms the previously reported association between blastocyst transfer and LGA babies, and shows a reduced risk of congenital anomaly following blastocyst transfer. Our sibling analysis did not confirm a decreased risk of low birthweight following blastocyst transfer. Overall, absolute risks are low and there is insufficient evidence to challenge the practice of extended culture of embryos.
Study funding/competing interests: This project is financed by an NHS Grampian Endowment Research Grant, project number 17/052. One of the authors, S.B., was the Editor in Chief of HROpen until 31 December 2022 and would have been in that role when the paper was first submitted. As an invited speaker, S.B. has received travel expenses, accommodation and honoraria from Merck, Organon, and Ferring. A.M. has received travel expenses, accommodation, and honoraria from Merck Serono, Cook Medical, Pharmasure, Gedeon Richter, and Ferring. D.J.M. is currently a HROpen Associate Editor.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


