Qing Yuan, Shanjuan Hong, Gregory Leya, Eve Roth, Georgios Tsoulfas, W W Williams, Joren C Madsen, Nahel Elias
{"title":"Analysis of the effects of donor and recipient hepatitis C infection on kidney transplant outcomes in the United States.","authors":"Qing Yuan, Shanjuan Hong, Gregory Leya, Eve Roth, Georgios Tsoulfas, W W Williams, Joren C Madsen, Nahel Elias","doi":"10.5500/wjt.v13.i2.44","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>As Hepatitis C virus infection (HCV+) rates in kidney donors and transplant recipients rise, direct-acting antivirals (DAA) may affect outcomes.</p><p><strong>Aim: </strong>To analyze the effects of HCV+ in donors, recipients, or both, on deceased-donor (DD) kidney transplantation (KT) outcomes, and the impact of DAAs on those effects.</p><p><strong>Methods: </strong>The Organ Procurement and Transplantation Network data of adult first solitary DD-KT recipients 1994-2019 were allocated into four groups by donor and recipient HCV+ status. We performed patient survival (PS) and death-censored graft survival (DCGS) pairwise comparisons after propensity score matching to assess the effects of HCV+ in donors and/or recipients, stratifying our study by DAA era to evaluate potential effect modification.</p><p><strong>Results: </strong>Pre-DAA, for HCV+ recipients, receiving an HCV+ kidney was associated with 1.28-fold higher mortality (HR <sub>1.15</sub>1.28<sub>1.42</sub>) and 1.22-fold higher death-censored graft failure (HR <sub>1.08</sub>1.22<sub>1.39</sub>) compared to receiving an HCV- kidney and the absolute risk difference was 3.3% (95%CI: 1.8%-4.7%) for PS and 3.1% (95%CI: 1.2%-5%) for DCGS at 3 years. The HCV dual-infection (donor plus recipient) group had worse PS (0.56-fold) and DCGS (0.71-fold) than the dual-uninfected. Donor HCV+ derived worse post-transplant outcomes than recipient HCV+ (PS 0.36-fold, DCGS 0.34-fold). In the DAA era, the risk associated with HCV+ in donors and/or recipients was no longer statistically significant, except for impaired PS in the dual-infected <i>vs</i> dual-uninfected (0.43-fold).</p><p><strong>Conclusion: </strong>Prior to DAA introduction, donor HCV+ negatively influenced kidney transplant outcomes in all recipients, while recipient infection only relatively impaired outcomes for uninfected donors. These adverse effects disappeared with the introduction of DAA.</p>","PeriodicalId":68893,"journal":{"name":"世界移植杂志(英文版)","volume":"13 2","pages":"44-57"},"PeriodicalIF":0.0000,"publicationDate":"2023-02-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0c/b8/WJT-13-44.PMC9993188.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"世界移植杂志(英文版)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5500/wjt.v13.i2.44","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Background: As Hepatitis C virus infection (HCV+) rates in kidney donors and transplant recipients rise, direct-acting antivirals (DAA) may affect outcomes.
Aim: To analyze the effects of HCV+ in donors, recipients, or both, on deceased-donor (DD) kidney transplantation (KT) outcomes, and the impact of DAAs on those effects.
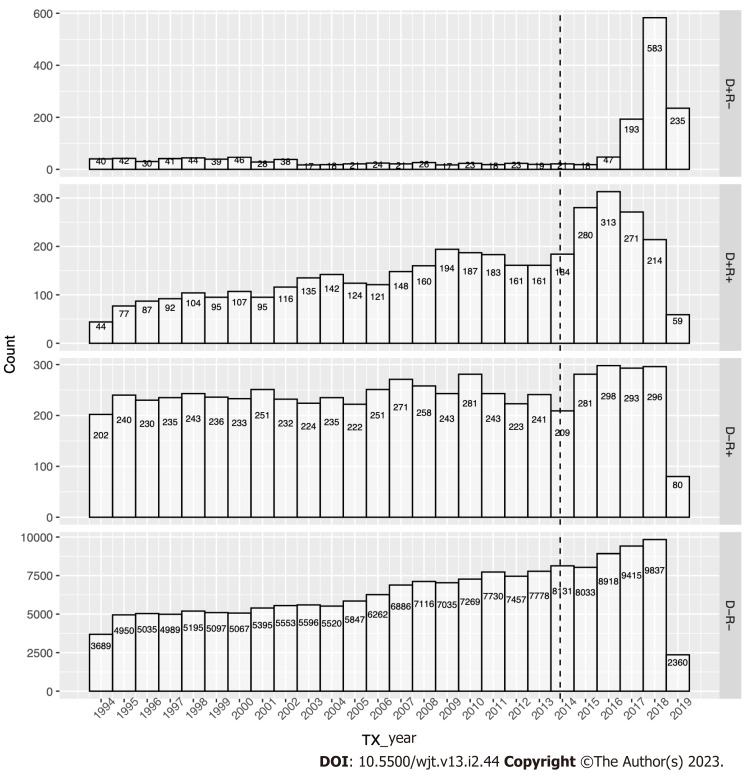
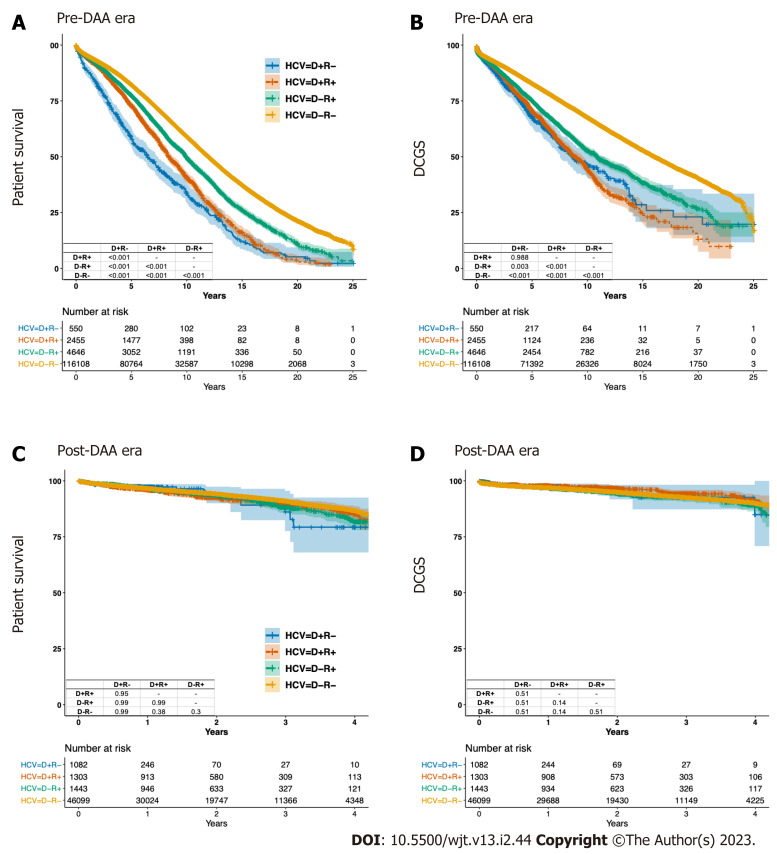
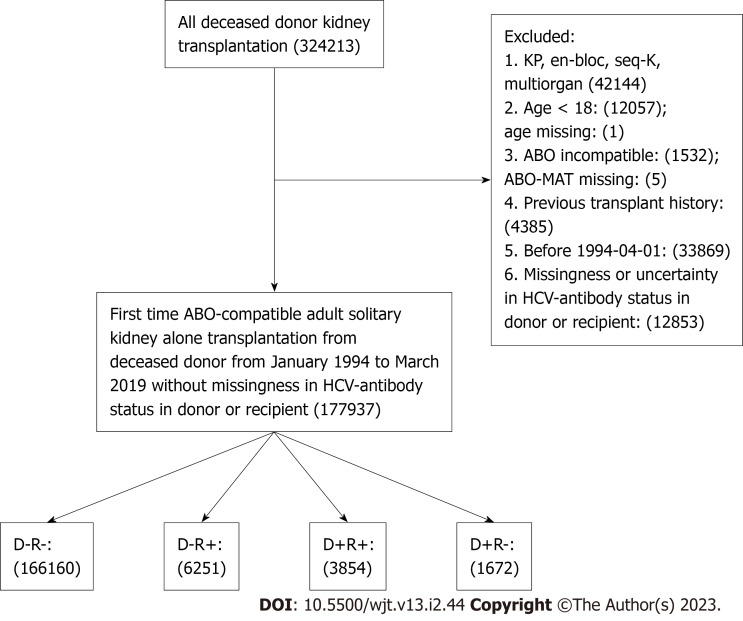
Methods: The Organ Procurement and Transplantation Network data of adult first solitary DD-KT recipients 1994-2019 were allocated into four groups by donor and recipient HCV+ status. We performed patient survival (PS) and death-censored graft survival (DCGS) pairwise comparisons after propensity score matching to assess the effects of HCV+ in donors and/or recipients, stratifying our study by DAA era to evaluate potential effect modification.
Results: Pre-DAA, for HCV+ recipients, receiving an HCV+ kidney was associated with 1.28-fold higher mortality (HR 1.151.281.42) and 1.22-fold higher death-censored graft failure (HR 1.081.221.39) compared to receiving an HCV- kidney and the absolute risk difference was 3.3% (95%CI: 1.8%-4.7%) for PS and 3.1% (95%CI: 1.2%-5%) for DCGS at 3 years. The HCV dual-infection (donor plus recipient) group had worse PS (0.56-fold) and DCGS (0.71-fold) than the dual-uninfected. Donor HCV+ derived worse post-transplant outcomes than recipient HCV+ (PS 0.36-fold, DCGS 0.34-fold). In the DAA era, the risk associated with HCV+ in donors and/or recipients was no longer statistically significant, except for impaired PS in the dual-infected vs dual-uninfected (0.43-fold).
Conclusion: Prior to DAA introduction, donor HCV+ negatively influenced kidney transplant outcomes in all recipients, while recipient infection only relatively impaired outcomes for uninfected donors. These adverse effects disappeared with the introduction of DAA.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


