Lewei Duan, Ming-Sum Lee, Jason N Doctor, John L Adams
{"title":"Addressing unmeasured confounding bias with a prior knowledge guided approach: coronary artery bypass grafting (CABG) versus percutaneous coronary intervention (PCI) in patients with stable ischemic heart disease.","authors":"Lewei Duan, Ming-Sum Lee, Jason N Doctor, John L Adams","doi":"10.1007/s10742-022-00282-y","DOIUrl":null,"url":null,"abstract":"<p><p>Unmeasured confounding undermines the validity of observational studies. Although randomized clinical trials (RCTs) are considered the \"gold standard\" of study types, we often observe divergent findings between RCTs and empirical settings. We present the \"L-table\", a simulation-based, prior knowledge (e.g., RCTs) guided approach that estimates the true effect adjusting for the potential influence of unmeasured confounders when using observational data. Using electronic health record data from Kaiser Permanente Southern California, we compare the effectiveness of coronary artery bypass grafting (CABG) and percutaneous coronary intervention (PCI) on endpoints at 1, 3, 5, and 10 years for patients with stable ischemic heart disease. We applied the L-table approach to the propensity score adjusted cohort to derive the omitted-confounder-adjusted estimated effects. After the L-table adjustment, CABG patients are 57.6% less likely to encounter major adverse cardiac and cerebrovascular event (MACCE) at 1 year (OR [95% CI] 0.424 [0.396, 0.517]), 56.4% less likely at 3 years (OR [95% CI] 0.436 [0.369, 0.527]), and 48.9% less likely at 5 years (OR [95% CI] 0.511 [0.451, 0.538]). CABG patients are also 49.5% less likely to die by the end of 10 years than PCI patients (OR [95% CI] 0.505 [0.446, 0.582]). We found the estimated true effects all shifted towards CABG as a more effective procedure that led to better health outcomes compared to PCI. Unlike existing sensitivity tools, the L-table approach explicitly lays out probable values and can therefore better support clinical decision-making. We recommend using L-table as a supplement to available techniques of sensitivity analysis.</p><p><strong>Supplementary information: </strong>The online version contains supplementary material available at 10.1007/s10742-022-00282-y.</p>","PeriodicalId":45600,"journal":{"name":"Health Services and Outcomes Research Methodology","volume":null,"pages":null},"PeriodicalIF":1.6000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9210342/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Services and Outcomes Research Methodology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s10742-022-00282-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
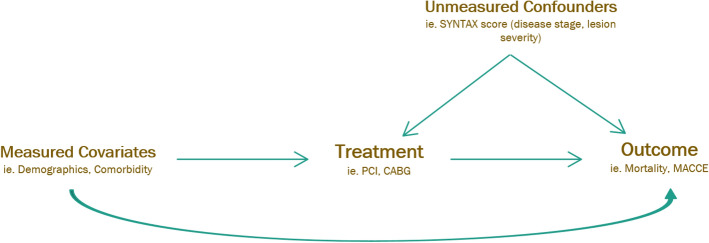
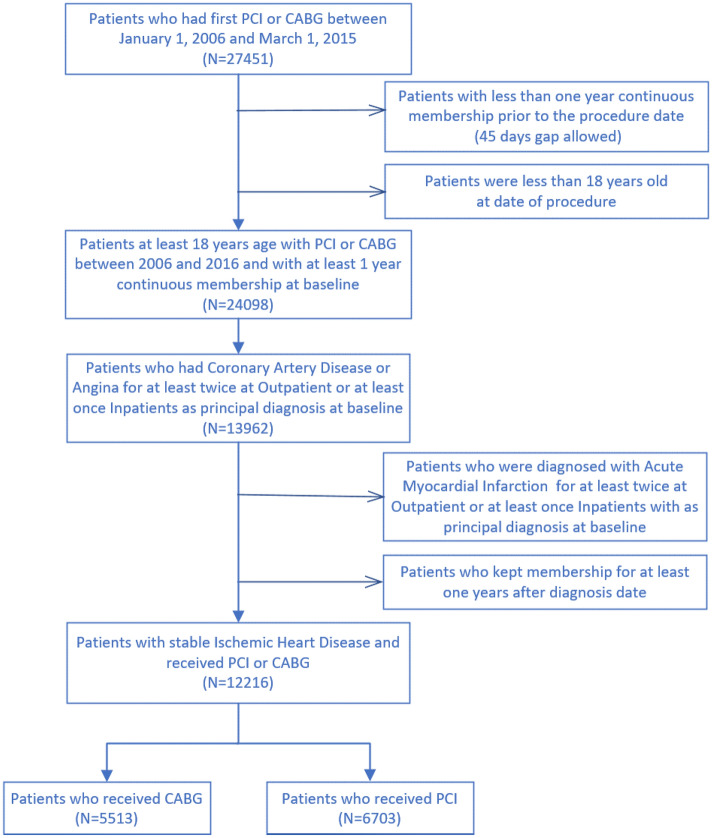
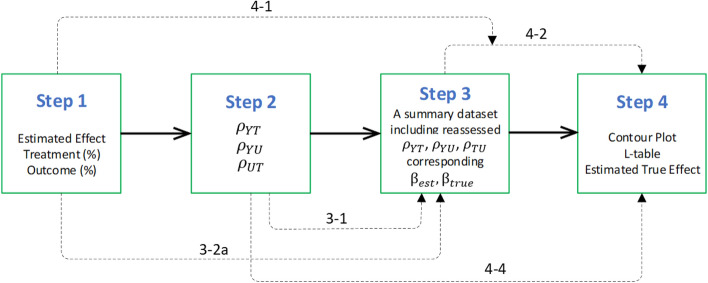
Unmeasured confounding undermines the validity of observational studies. Although randomized clinical trials (RCTs) are considered the "gold standard" of study types, we often observe divergent findings between RCTs and empirical settings. We present the "L-table", a simulation-based, prior knowledge (e.g., RCTs) guided approach that estimates the true effect adjusting for the potential influence of unmeasured confounders when using observational data. Using electronic health record data from Kaiser Permanente Southern California, we compare the effectiveness of coronary artery bypass grafting (CABG) and percutaneous coronary intervention (PCI) on endpoints at 1, 3, 5, and 10 years for patients with stable ischemic heart disease. We applied the L-table approach to the propensity score adjusted cohort to derive the omitted-confounder-adjusted estimated effects. After the L-table adjustment, CABG patients are 57.6% less likely to encounter major adverse cardiac and cerebrovascular event (MACCE) at 1 year (OR [95% CI] 0.424 [0.396, 0.517]), 56.4% less likely at 3 years (OR [95% CI] 0.436 [0.369, 0.527]), and 48.9% less likely at 5 years (OR [95% CI] 0.511 [0.451, 0.538]). CABG patients are also 49.5% less likely to die by the end of 10 years than PCI patients (OR [95% CI] 0.505 [0.446, 0.582]). We found the estimated true effects all shifted towards CABG as a more effective procedure that led to better health outcomes compared to PCI. Unlike existing sensitivity tools, the L-table approach explicitly lays out probable values and can therefore better support clinical decision-making. We recommend using L-table as a supplement to available techniques of sensitivity analysis.
Supplementary information: The online version contains supplementary material available at 10.1007/s10742-022-00282-y.
期刊介绍:
The journal reflects the multidisciplinary nature of the field of health services and outcomes research. It addresses the needs of multiple, interlocking communities, including methodologists in statistics, econometrics, social and behavioral sciences; designers and analysts of health policy and health services research projects; and health care providers and policy makers who need to properly understand and evaluate the results of published research. The journal strives to enhance the level of methodologic rigor in health services and outcomes research and contributes to the development of methodologic standards in the field. In pursuing its main objective, the journal also provides a meeting ground for researchers from a number of traditional disciplines and fosters the development of new quantitative, qualitative, and mixed methods by statisticians, econometricians, health services researchers, and methodologists in other fields. Health Services and Outcomes Research Methodology publishes: Research papers on quantitative, qualitative, and mixed methods; Case Studies describing applications of quantitative and qualitative methodology in health services and outcomes research; Review Articles synthesizing and popularizing methodologic developments; Tutorials; Articles on computational issues and software reviews; Book reviews; and Notices. Special issues will be devoted to papers presented at important workshops and conferences.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


