Patrícia Pita Ferreira, Diogo Godinho Simões, Constança Pinto de Carvalho, Francisco Duarte, Eugénia Fernandes, Pedro Casaca Carvalho, José Francisco Loff, Ana Paula Soares, Maria João Albuquerque, Pedro Pinto-Leite, André Peralta-Santos
{"title":"Real-Time Classification of Causes of Death Using AI: Sensitivity Analysis.","authors":"Patrícia Pita Ferreira, Diogo Godinho Simões, Constança Pinto de Carvalho, Francisco Duarte, Eugénia Fernandes, Pedro Casaca Carvalho, José Francisco Loff, Ana Paula Soares, Maria João Albuquerque, Pedro Pinto-Leite, André Peralta-Santos","doi":"10.2196/40965","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In 2021, the European Union reported >270,000 excess deaths, including >16,000 in Portugal. The Portuguese Directorate-General of Health developed a deep neural network, AUTOCOD, which determines the primary causes of death by analyzing the free text of physicians' death certificates (DCs). Although AUTOCOD's performance has been established, it remains unclear whether its performance remains consistent over time, particularly during periods of excess mortality.</p><p><strong>Objective: </strong>This study aims to assess the sensitivity and other performance metrics of AUTOCOD in classifying underlying causes of death compared with manual coding to identify specific causes of death during periods of excess mortality.</p><p><strong>Methods: </strong>We included all DCs between 2016 and 2019. AUTOCOD's performance was evaluated by calculating various performance metrics, such as sensitivity, specificity, positive predictive value (PPV), and F<sub>1</sub>-score, using a confusion matrix. This compared International Statistical Classification of Diseases and Health-Related Problems, 10th Revision (ICD-10), classifications of DCs by AUTOCOD with those by human coders at the Directorate-General of Health (gold standard). Subsequently, we compared periods without excess mortality with periods of excess, severe, and extreme excess mortality. We defined excess mortality as 2 consecutive days with a Z score above the 95% baseline limit, severe excess mortality as 2 consecutive days with a Z score >4 SDs, and extreme excess mortality as 2 consecutive days with a Z score >6 SDs. Finally, we repeated the analyses for the 3 most common ICD-10 chapters focusing on block-level classification.</p><p><strong>Results: </strong>We analyzed a large data set comprising 330,098 DCs classified by both human coders and AUTOCOD. AUTOCOD demonstrated high sensitivity (≥0.75) for 10 ICD-10 chapters examined, with values surpassing 0.90 for the more prevalent chapters (chapter II-\"Neoplasms,\" chapter IX-\"Diseases of the circulatory system,\" and chapter X-\"Diseases of the respiratory system\"), accounting for 67.69% (223,459/330,098) of all human-coded causes of death. No substantial differences were observed in these high-sensitivity values when comparing periods without excess mortality with periods of excess, severe, and extreme excess mortality. The same holds for specificity, which exceeded 0.96 for all chapters examined, and for PPV, which surpassed 0.75 in 9 chapters, including the more prevalent ones. When considering block classification within the 3 most common ICD-10 chapters, AUTOCOD maintained a high performance, demonstrating high sensitivity (≥0.75) for 13 ICD-10 blocks, high PPV for 9 blocks, and specificity of >0.98 in all blocks, with no significant differences between periods without excess mortality and those with excess mortality.</p><p><strong>Conclusions: </strong>Our findings indicate that, during periods of excess and extreme excess mortality, AUTOCOD's performance remains unaffected by potential text quality degradation because of pressure on health services. Consequently, AUTOCOD can be dependably used for real-time cause-specific mortality surveillance even in extreme excess mortality situations.</p>","PeriodicalId":50817,"journal":{"name":"American Fern Journal","volume":"63 1","pages":"e40965"},"PeriodicalIF":0.9000,"publicationDate":"2023-11-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11041420/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Fern Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/40965","RegionNum":4,"RegionCategory":"生物学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PLANT SCIENCES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In 2021, the European Union reported >270,000 excess deaths, including >16,000 in Portugal. The Portuguese Directorate-General of Health developed a deep neural network, AUTOCOD, which determines the primary causes of death by analyzing the free text of physicians' death certificates (DCs). Although AUTOCOD's performance has been established, it remains unclear whether its performance remains consistent over time, particularly during periods of excess mortality.
Objective: This study aims to assess the sensitivity and other performance metrics of AUTOCOD in classifying underlying causes of death compared with manual coding to identify specific causes of death during periods of excess mortality.
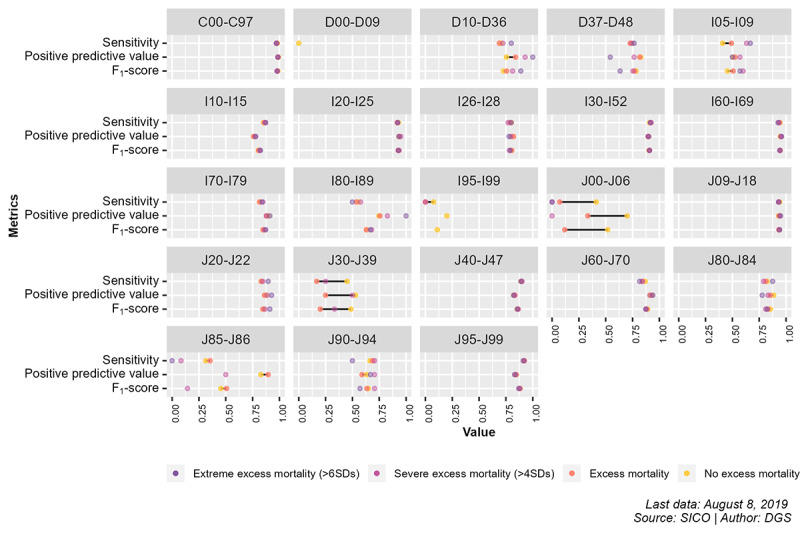
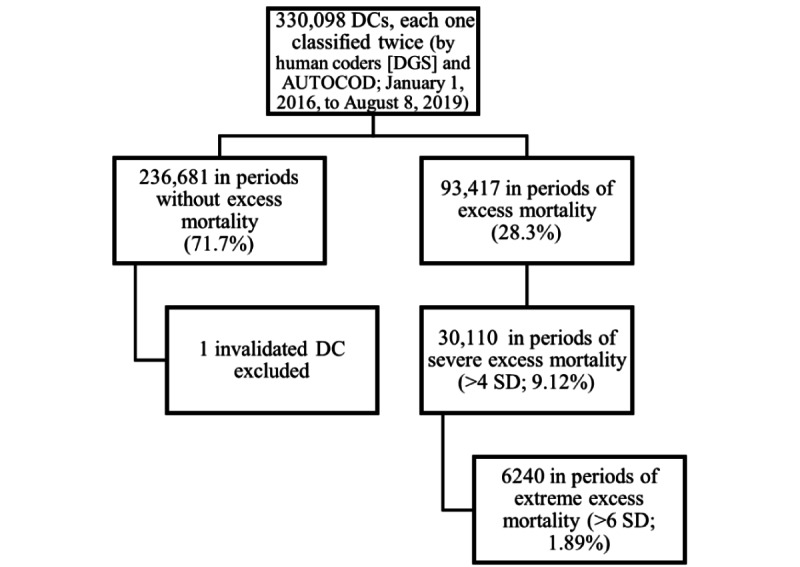
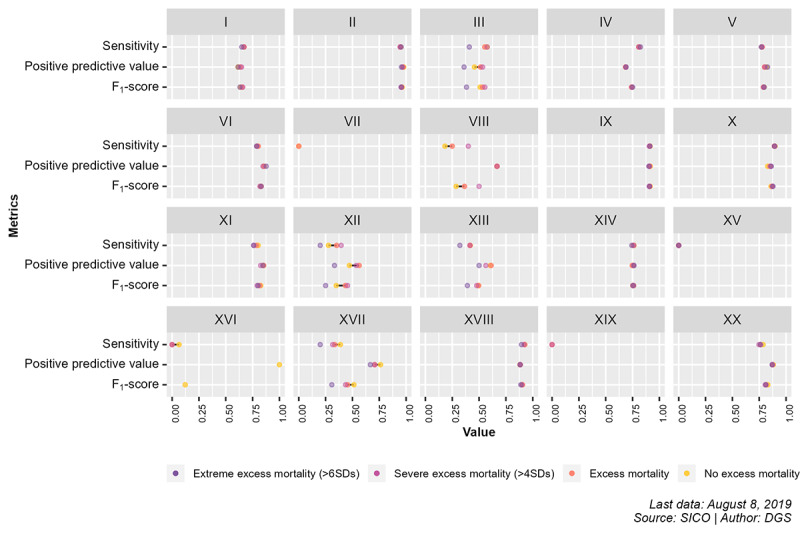
Methods: We included all DCs between 2016 and 2019. AUTOCOD's performance was evaluated by calculating various performance metrics, such as sensitivity, specificity, positive predictive value (PPV), and F1-score, using a confusion matrix. This compared International Statistical Classification of Diseases and Health-Related Problems, 10th Revision (ICD-10), classifications of DCs by AUTOCOD with those by human coders at the Directorate-General of Health (gold standard). Subsequently, we compared periods without excess mortality with periods of excess, severe, and extreme excess mortality. We defined excess mortality as 2 consecutive days with a Z score above the 95% baseline limit, severe excess mortality as 2 consecutive days with a Z score >4 SDs, and extreme excess mortality as 2 consecutive days with a Z score >6 SDs. Finally, we repeated the analyses for the 3 most common ICD-10 chapters focusing on block-level classification.
Results: We analyzed a large data set comprising 330,098 DCs classified by both human coders and AUTOCOD. AUTOCOD demonstrated high sensitivity (≥0.75) for 10 ICD-10 chapters examined, with values surpassing 0.90 for the more prevalent chapters (chapter II-"Neoplasms," chapter IX-"Diseases of the circulatory system," and chapter X-"Diseases of the respiratory system"), accounting for 67.69% (223,459/330,098) of all human-coded causes of death. No substantial differences were observed in these high-sensitivity values when comparing periods without excess mortality with periods of excess, severe, and extreme excess mortality. The same holds for specificity, which exceeded 0.96 for all chapters examined, and for PPV, which surpassed 0.75 in 9 chapters, including the more prevalent ones. When considering block classification within the 3 most common ICD-10 chapters, AUTOCOD maintained a high performance, demonstrating high sensitivity (≥0.75) for 13 ICD-10 blocks, high PPV for 9 blocks, and specificity of >0.98 in all blocks, with no significant differences between periods without excess mortality and those with excess mortality.
Conclusions: Our findings indicate that, during periods of excess and extreme excess mortality, AUTOCOD's performance remains unaffected by potential text quality degradation because of pressure on health services. Consequently, AUTOCOD can be dependably used for real-time cause-specific mortality surveillance even in extreme excess mortality situations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


