Tonic-Clonic Seizure in Patient With SLE: Posterior Reversible Encephalopathy Syndrome, or a Neuropsychiatric Manifestation of SLE?
Q4 Medicine
Mediterranean Journal of Rheumatology
Pub Date : 2023-09-05
eCollection Date: 2023-09-01
DOI:10.31138/mjr.20230905.tc
引用次数: 0
Abstract
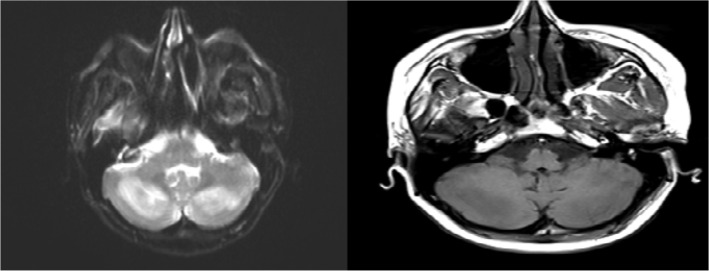
Posterior reversible encephalopathy syndrome (PRES) is a clinically and radiologically diagnosed reversible sudden onset disease with many neurological symptoms. SLE is the most common cause of PRES among autoimmune diseases. Many factors, such as SLE activity, hypertension, hematological and renal diseases, lymphopenia dyslipidemia, and immunosuppressive treatments, can trigger PRES in SLE. We wanted to draw attention to the difference between neuropsychiatric systemic lupus erythematosus (SLE) and PRES in a patient with SLE and the triggers for developing PRES in SLE by presenting a hypertensive patient on immunosuppressive therapy who had just started haemodialysis treatment and had generalised tonic-clonic seizures.
SLE患者强直性脊柱炎发作:SLE的后发可逆性脑病综合征还是神经精神表现?
后部可逆性脑病综合征(PRES)是一种临床和放射学诊断的可逆性突发疾病,具有许多神经系统症状。SLE是自身免疫性疾病中最常见的PRES病因。许多因素,如SLE活动、高血压、血液学和肾脏疾病、淋巴细胞减少症、血脂异常和免疫抑制治疗,都可以触发SLE的PRES。我们想通过向一名刚刚开始血液透析治疗并出现全身强直-阵挛发作的接受免疫抑制治疗的高血压患者介绍神经精神系统性红斑狼疮(SLE)和SLE患者的PRES之间的差异,以及在SLE中发生PRES的诱因。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

Mediterranean Journal of Rheumatology
Medicine-Rheumatology
CiteScore
2.00
自引率
0.00%
发文量
42
审稿时长
8 weeks
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


