Door-to-device time and mortality in patients with ST-elevation myocardial infarction treated with primary percutaneous coronary intervention: insight from real world data of Thai PCI Registry.
{"title":"Door-to-device time and mortality in patients with ST-elevation myocardial infarction treated with primary percutaneous coronary intervention: insight from real world data of Thai PCI Registry.","authors":"Kitcha Champasri, Suphot Srimahachota, Mann Chandavimol, Wasan Udayachalerm, Ammarin Thakkinstian, Bancha Sookananchai, Wannakorn Phatharajaree, Songsak Kiatchoosakun, Nakarin Sansanayudh","doi":"10.21037/cdt-22-611","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Timely reperfusion therapy is recommended for patients with ST-segment elevation myocardial infarction (STEMI), and system delay <90 minutes and door-to-device (D2D) time <60 minutes are recommended by the 2017 ESC Guidelines for the management of STEMI patients and have been proposed as a performance measure for triaging patients for primary percutaneous coronary intervention (PCI). However, previous research produced contradictory results regarding the association between D2D time and mortality. Therefore, this study aimed to examine the associations between D2D time and mortality in Thailand.</p><p><strong>Methods: </strong>This cohort study included STEMI patients treated with primary PCI in 39 PCI centres in Thailand from February 27, 2018, to August 1, 2019. Patients were eligible if they met the following criteria: primary STEMI diagnosis, symptom onset within 12 hours, and ST-segment elevation of at least 0.1 mV in 2 or more contiguous leads (at least 0.2 mV in V1-V3) or a new left bundle branch block.</p><p><strong>Results: </strong>Within 12 hours of symptom onset, 3,874 patients underwent primary PCI. The median D2D time was 54 minutes [interquartile range (IQR) 29-90], and there was a significant difference between patients transferred from other hospitals (44 minutes, IQR 25-77, n=2,871) and patients presented directly to PCI centres (81 minutes, IQR 56-129, n=1,003) (P<0.001). Overall, in-hospital mortality was 7.8%. In a multivariable analysis, adjusting for other predictors of mortality and stratifying according to intervals of D2D time, cumulative in-hospital mortality was significantly higher in patients with a D2D time greater than 90 minutes [hazard ratio (HR) 1.5, 95% confidence interval (CI): 1.0-2.1, P=0.046] but not associated with D2D time shorter than 60 minutes (HR 1.2, 95% CI: 0.8-1.8, P=0.319).</p><p><strong>Conclusions: </strong>A D2D time greater than 90 minutes was related to in-hospital mortality in patients with STEMI treated with primary PCI, but a D2D time less than 60 minutes was not consistently associated with D2D time-improved survival in real-world, contemporary practice in Thailand.</p>","PeriodicalId":9592,"journal":{"name":"Cardiovascular diagnosis and therapy","volume":"13 5","pages":"843-854"},"PeriodicalIF":2.1000,"publicationDate":"2023-10-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10628423/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiovascular diagnosis and therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/cdt-22-611","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/10/8 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
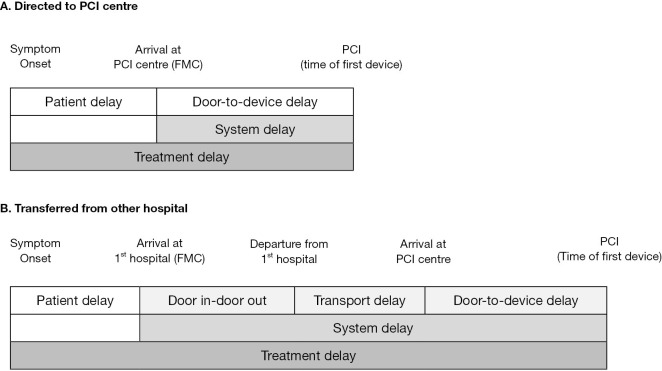
Background: Timely reperfusion therapy is recommended for patients with ST-segment elevation myocardial infarction (STEMI), and system delay <90 minutes and door-to-device (D2D) time <60 minutes are recommended by the 2017 ESC Guidelines for the management of STEMI patients and have been proposed as a performance measure for triaging patients for primary percutaneous coronary intervention (PCI). However, previous research produced contradictory results regarding the association between D2D time and mortality. Therefore, this study aimed to examine the associations between D2D time and mortality in Thailand.
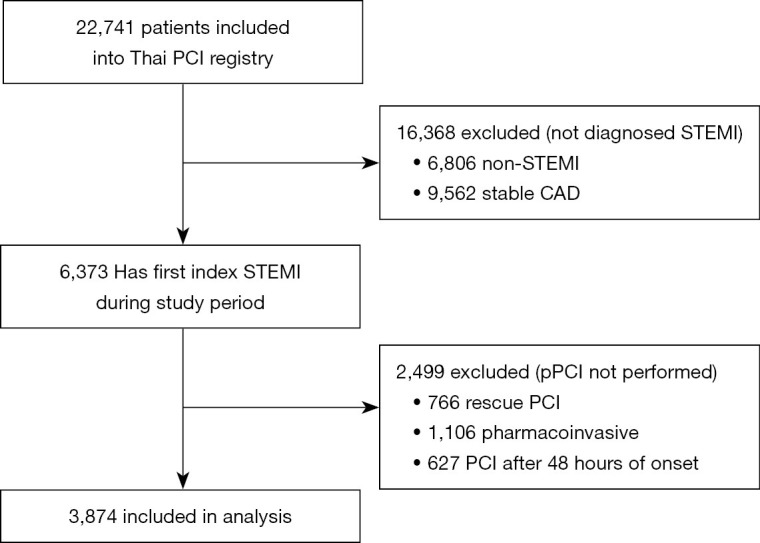
Methods: This cohort study included STEMI patients treated with primary PCI in 39 PCI centres in Thailand from February 27, 2018, to August 1, 2019. Patients were eligible if they met the following criteria: primary STEMI diagnosis, symptom onset within 12 hours, and ST-segment elevation of at least 0.1 mV in 2 or more contiguous leads (at least 0.2 mV in V1-V3) or a new left bundle branch block.
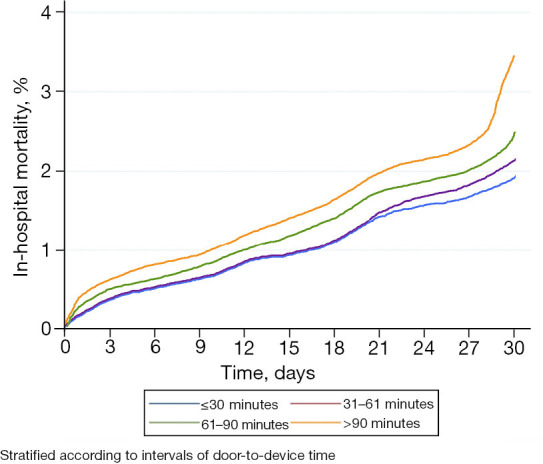
Results: Within 12 hours of symptom onset, 3,874 patients underwent primary PCI. The median D2D time was 54 minutes [interquartile range (IQR) 29-90], and there was a significant difference between patients transferred from other hospitals (44 minutes, IQR 25-77, n=2,871) and patients presented directly to PCI centres (81 minutes, IQR 56-129, n=1,003) (P<0.001). Overall, in-hospital mortality was 7.8%. In a multivariable analysis, adjusting for other predictors of mortality and stratifying according to intervals of D2D time, cumulative in-hospital mortality was significantly higher in patients with a D2D time greater than 90 minutes [hazard ratio (HR) 1.5, 95% confidence interval (CI): 1.0-2.1, P=0.046] but not associated with D2D time shorter than 60 minutes (HR 1.2, 95% CI: 0.8-1.8, P=0.319).
Conclusions: A D2D time greater than 90 minutes was related to in-hospital mortality in patients with STEMI treated with primary PCI, but a D2D time less than 60 minutes was not consistently associated with D2D time-improved survival in real-world, contemporary practice in Thailand.
期刊介绍:
The journal ''Cardiovascular Diagnosis and Therapy'' (Print ISSN: 2223-3652; Online ISSN: 2223-3660) accepts basic and clinical science submissions related to Cardiovascular Medicine and Surgery. The mission of the journal is the rapid exchange of scientific information between clinicians and scientists worldwide. To reach this goal, the journal will focus on novel media, using a web-based, digital format in addition to traditional print-version. This includes on-line submission, review, publication, and distribution. The digital format will also allow submission of extensive supporting visual material, both images and video. The website www.thecdt.org will serve as the central hub and also allow posting of comments and on-line discussion. The web-site of the journal will be linked to a number of international web-sites (e.g. www.dxy.cn), which will significantly expand the distribution of its contents.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


