{"title":"Immune checkpoint inhibitors plus chemotherapy for HER2-negative advanced gastric/gastroesophageal junction cancer: a cost-effectiveness analysis.","authors":"Youwen Zhu, Kun Liu, Hong Zhu, Haijun Wu","doi":"10.1177/17562848231207200","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Nivolumab plus chemotherapy (NC) was recently approved as the first-line intervention for human epidermal growth factor receptor 2-negative advanced gastric/gastroesophageal junction cancer (GC/GEJC). Moreover, in the latest KEYNOTE-859 (NCT03675737), pembrolizumab plus chemotherapy (PC) was demonstrated to produce remarkable patient survival outcomes.</p><p><strong>Objectives: </strong>The clinicians and patients need to assess NC and PC preference for cancer drugs.</p><p><strong>Design: </strong>The cost-effective analysis.</p><p><strong>Methods: </strong>In an economic assessment of the United States, United Kingdom, and Chinese healthcare systems using a Markov model simulated patients with GC/GEJC, two treatment decision branches with three health states and a tracked time horizon of 15 years were developed. The overall cost and efficacy outcomes of first-line strategies PC and NC were evaluated at willingness-to-pay (WTP) thresholds of different national, including life-years (LYs), quality-adjusted life-years (QALYs), incremental cost-effectiveness ratios (ICERs), and incremental net-health benefit (INHB). Sensitivity and subgroup analyses were considered.</p><p><strong>Results: </strong>Given a WTP threshold of $150,000, $60,161, and $37,653 per QALY in the United States, United Kingdom, and China, respectively, both PC and NC achieved QALYs of 1.67 and 1.65 (2.51 and 2.48 LYs), 1.65 and 1.63 (2.48 and 2.45 LYs), and 1.60 and 1.58 (2.40 and 2.37 LYs), with total costs of $242,444 and $232,617, $148,367 and $127,737, and $16,693 and $24,016, respectively. Based on our sensitivity analysis, the programmed death-1 inhibitors cost produced the largest impact on the outcome. In addition, the cost-effectiveness probabilities of PC were 38.3%, 4.1%, and 100% in the three aforementioned countries, respectively.</p><p><strong>Conclusion: </strong>In the case of the Chinese payers' perspective, PC appeared more dominant as first-line therapy for advanced GC/GEJC patients, whereas NC was preferred in the United States and United Kingdom.</p>","PeriodicalId":48770,"journal":{"name":"Therapeutic Advances in Gastroenterology","volume":"16 ","pages":"17562848231207200"},"PeriodicalIF":3.9000,"publicationDate":"2023-11-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10624011/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17562848231207200","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Nivolumab plus chemotherapy (NC) was recently approved as the first-line intervention for human epidermal growth factor receptor 2-negative advanced gastric/gastroesophageal junction cancer (GC/GEJC). Moreover, in the latest KEYNOTE-859 (NCT03675737), pembrolizumab plus chemotherapy (PC) was demonstrated to produce remarkable patient survival outcomes.
Objectives: The clinicians and patients need to assess NC and PC preference for cancer drugs.
Design: The cost-effective analysis.
Methods: In an economic assessment of the United States, United Kingdom, and Chinese healthcare systems using a Markov model simulated patients with GC/GEJC, two treatment decision branches with three health states and a tracked time horizon of 15 years were developed. The overall cost and efficacy outcomes of first-line strategies PC and NC were evaluated at willingness-to-pay (WTP) thresholds of different national, including life-years (LYs), quality-adjusted life-years (QALYs), incremental cost-effectiveness ratios (ICERs), and incremental net-health benefit (INHB). Sensitivity and subgroup analyses were considered.
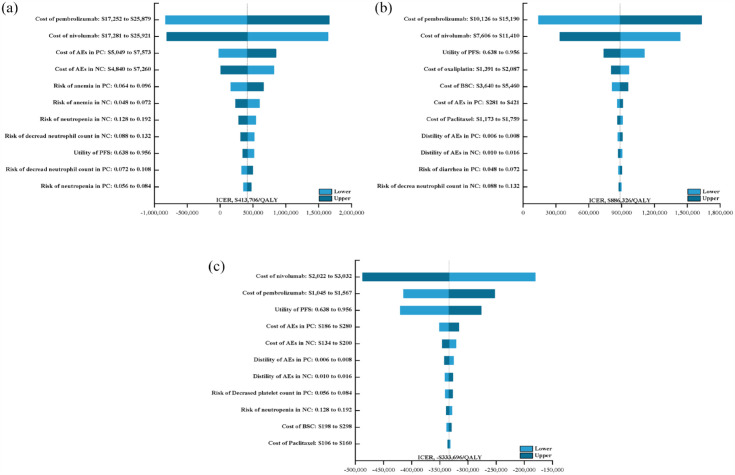
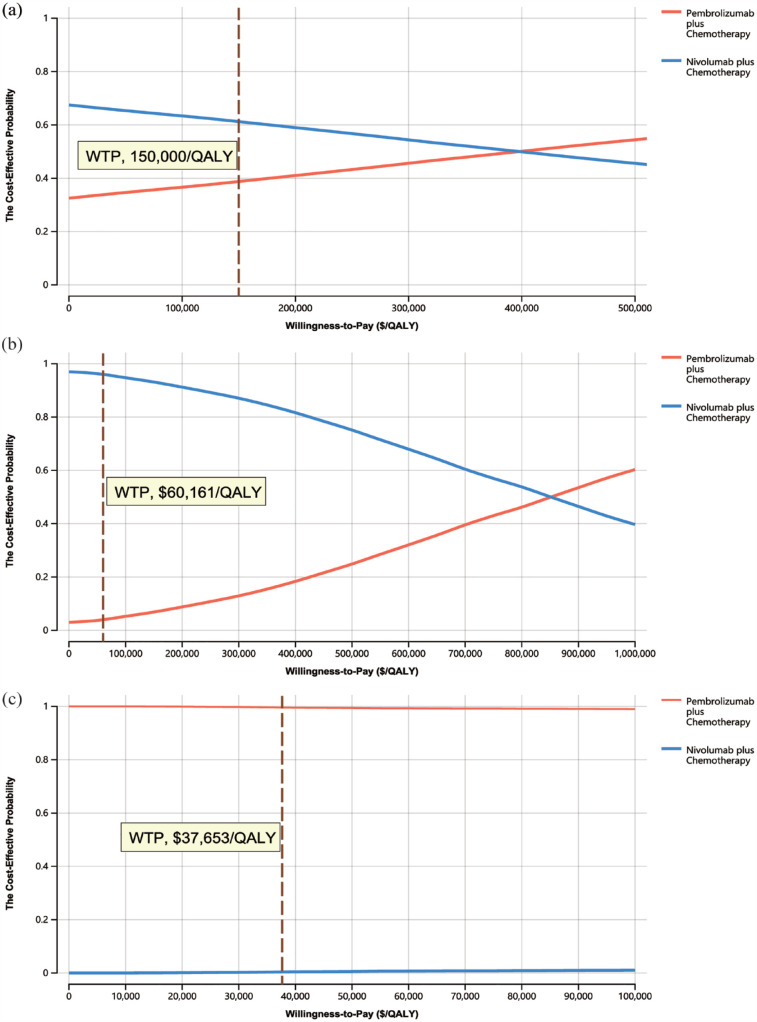
Results: Given a WTP threshold of $150,000, $60,161, and $37,653 per QALY in the United States, United Kingdom, and China, respectively, both PC and NC achieved QALYs of 1.67 and 1.65 (2.51 and 2.48 LYs), 1.65 and 1.63 (2.48 and 2.45 LYs), and 1.60 and 1.58 (2.40 and 2.37 LYs), with total costs of $242,444 and $232,617, $148,367 and $127,737, and $16,693 and $24,016, respectively. Based on our sensitivity analysis, the programmed death-1 inhibitors cost produced the largest impact on the outcome. In addition, the cost-effectiveness probabilities of PC were 38.3%, 4.1%, and 100% in the three aforementioned countries, respectively.
Conclusion: In the case of the Chinese payers' perspective, PC appeared more dominant as first-line therapy for advanced GC/GEJC patients, whereas NC was preferred in the United States and United Kingdom.
期刊介绍:
Therapeutic Advances in Gastroenterology is an open access journal which delivers the highest quality peer-reviewed original research articles, reviews, and scholarly comment on pioneering efforts and innovative studies in the medical treatment of gastrointestinal and hepatic disorders. The journal has a strong clinical and pharmacological focus and is aimed at an international audience of clinicians and researchers in gastroenterology and related disciplines, providing an online forum for rapid dissemination of recent research and perspectives in this area.
The editors welcome original research articles across all areas of gastroenterology and hepatology.
The journal publishes original research articles and review articles primarily. Original research manuscripts may include laboratory, animal or human/clinical studies – all phases. Letters to the Editor and Case Reports will also be considered.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


