Hoi Ying Sharon Lau, Xuelian Wang, Ho Tsun Michelia Wong, Ka Hei Catherine Lam, Hugh Simon Lam
{"title":"Enhanced Category-Based Risk Assessment for Neonatal Early-Onset Sepsis: A Prospective Observational Study.","authors":"Hoi Ying Sharon Lau, Xuelian Wang, Ho Tsun Michelia Wong, Ka Hei Catherine Lam, Hugh Simon Lam","doi":"10.1159/000534091","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Compared with multivariate risk assessment, traditional category-based risk assessment (CRA) approaches for neonatal early-onset sepsis (EOS) screening are usually straightforward to use, do not require electronic devices, but are associated with higher rates of antibiotic use. This study aims to evaluate the performance of a novel enhanced CRA (eCRA) framework on EOS admissions and antibiotic use and to investigate whether a modified version with adjustments in risk factor weighting can allow its performance to match the EOS calculator while remaining easy to implement.</p><p><strong>Method: </strong>This is a prospective, single-center, two-phase observational study. Infants of all gestations delivered in a tertiary hospital in Hong Kong with risk factors or clinical features of EOS were recruited.</p><p><strong>Phase i: </strong>A novel eCRA framework (period 2) was compared with the CDC 2010-based protocol (period 1).</p><p><strong>Phase ii: </strong>A modified eCRA framework was compared theoretically with the EOS calculator. EOS-specific admissions and antibiotic use were measured.</p><p><strong>Results: </strong>Phase I: 1,025 at-risk infants were recruited during period 2 and compared with 757 infants of period 1. Admissions and antibiotic use decreased from 45.8% to 29.4% and 41.1% to 28.2%, respectively. Antibiotics among those at-risk but well-appearing infants decreased from 25.3% to 16.3% (p < 0.001 for all).</p><p><strong>Phase ii: </strong>antibiotic use was similar (7.3 vs. 6.4%, p = 0.42) between the modified eCRA framework and the EOS calculator.</p><p><strong>Conclusions: </strong>An eCRA framework can effectively and safely provide individualized guidance for EOS screening without the need for tools such as the EOS calculator.</p>","PeriodicalId":94152,"journal":{"name":"Neonatology","volume":" ","pages":"56-64"},"PeriodicalIF":3.0000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10836755/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neonatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000534091","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/10/31 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
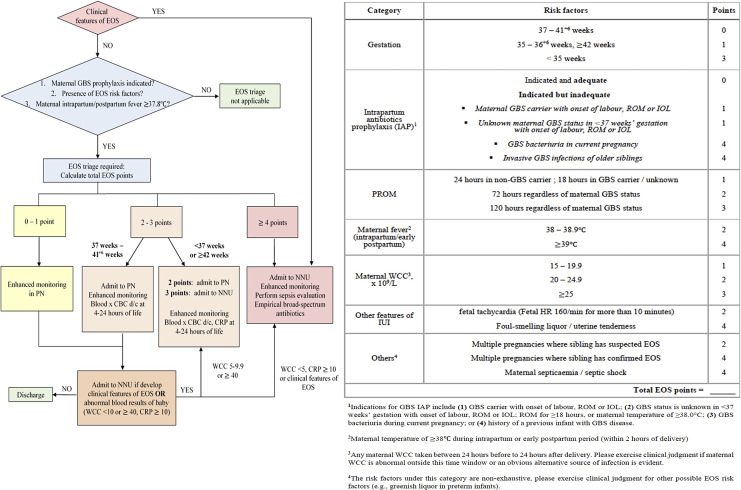
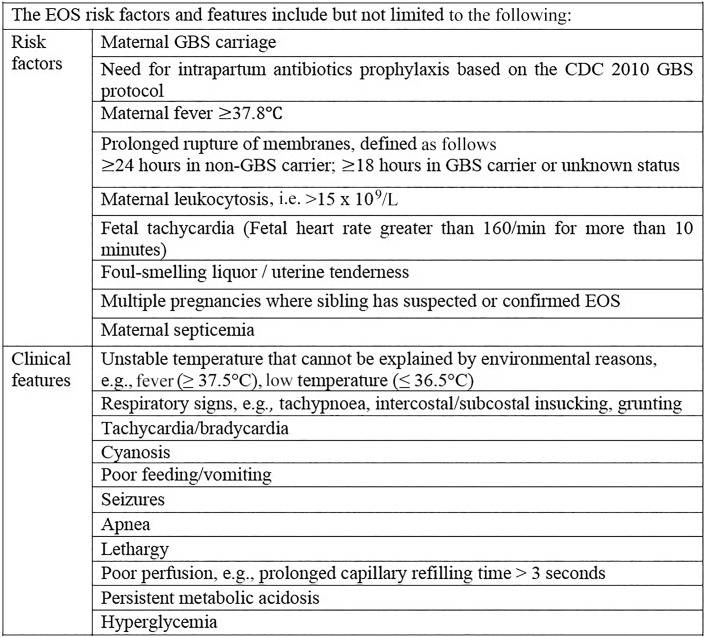
Introduction: Compared with multivariate risk assessment, traditional category-based risk assessment (CRA) approaches for neonatal early-onset sepsis (EOS) screening are usually straightforward to use, do not require electronic devices, but are associated with higher rates of antibiotic use. This study aims to evaluate the performance of a novel enhanced CRA (eCRA) framework on EOS admissions and antibiotic use and to investigate whether a modified version with adjustments in risk factor weighting can allow its performance to match the EOS calculator while remaining easy to implement.
Method: This is a prospective, single-center, two-phase observational study. Infants of all gestations delivered in a tertiary hospital in Hong Kong with risk factors or clinical features of EOS were recruited.
Phase i: A novel eCRA framework (period 2) was compared with the CDC 2010-based protocol (period 1).
Phase ii: A modified eCRA framework was compared theoretically with the EOS calculator. EOS-specific admissions and antibiotic use were measured.
Results: Phase I: 1,025 at-risk infants were recruited during period 2 and compared with 757 infants of period 1. Admissions and antibiotic use decreased from 45.8% to 29.4% and 41.1% to 28.2%, respectively. Antibiotics among those at-risk but well-appearing infants decreased from 25.3% to 16.3% (p < 0.001 for all).
Phase ii: antibiotic use was similar (7.3 vs. 6.4%, p = 0.42) between the modified eCRA framework and the EOS calculator.
Conclusions: An eCRA framework can effectively and safely provide individualized guidance for EOS screening without the need for tools such as the EOS calculator.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


