Elsadig Hussan, Alexander Kroemer, Ahmed M Elsabbagh, Khalid M Khan, Nada A Yazigi, Udeme D Ekong, Sukanya Subramanian, Shahira S Ghobrial, Juan-Francisco Guerra, Thomas M Fishbein, Cal S Matsumoto, Stuart S Kaufman
{"title":"Idiopathic Ileal Ulceration After Intestinal Transplantation.","authors":"Elsadig Hussan, Alexander Kroemer, Ahmed M Elsabbagh, Khalid M Khan, Nada A Yazigi, Udeme D Ekong, Sukanya Subramanian, Shahira S Ghobrial, Juan-Francisco Guerra, Thomas M Fishbein, Cal S Matsumoto, Stuart S Kaufman","doi":"10.1097/TXD.0000000000001529","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Idiopathic ileal ulceration after intestinal transplantation (ITx) has been discussed infrequently and has an uncertain natural history and relation to graft rejection. Herein, we review our experience with this pathology.</p><p><strong>Methods: </strong>We retrospectively reviewed 225 ITx in 217 patients with minimum 1 y graft survival. Routine graft endoscopy was conducted up to twice weekly within the first 90 d after ITx, gradually decreasing to once yearly. Risks for ulceration over time were evaluated using Cox regression.</p><p><strong>Results: </strong>Of 93 (41%) patients with ulcers, 50 were found within 90 d after ITx mostly via ileoscopy; delayed healing after biopsy appeared causal in the majority. Of the remaining 43 patients with ulcers found >90 d after ITx, 36 were after ileostomy closure. Multivariable modeling demonstrated within 90-d ulcer associations with increasing patient age (hazard ratio [HR], 1.027; <i>P</i> < 0.001) and loop ileostomy (versus Santulli ileostomy; HR, 0.271; <i>P</i> < 0.001). For ulcers appearing after ileostomy closure, their sole association was with absence of graft colon (HR, 7.232; <i>P</i> < 0.001). For ulcers requiring extended anti-microbial and anti-inflammatory therapy, associations included de novo donor-specific antibodies (HR, 3.222; <i>P</i> < 0.007) and nucleotide oligomerization domain mutations (HR, 2.772; <i>P</i> < 0.016). Whole-cohort post-ITx ulceration was not associated with either graft rejection (<i>P</i> = 0.161) or graft failure (<i>P</i> = 0.410).</p><p><strong>Conclusions: </strong>Idiopathic ulceration after ITx is relatively common but has little independent influence on outcome; risks include ileostomy construction, colon-free ITx, immunologic mutation, and donor sensitization.</p>","PeriodicalId":23225,"journal":{"name":"Transplantation Direct","volume":"9 11","pages":"e1529"},"PeriodicalIF":1.9000,"publicationDate":"2023-10-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10602531/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation Direct","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/TXD.0000000000001529","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/11/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
引用次数: 0
Abstract
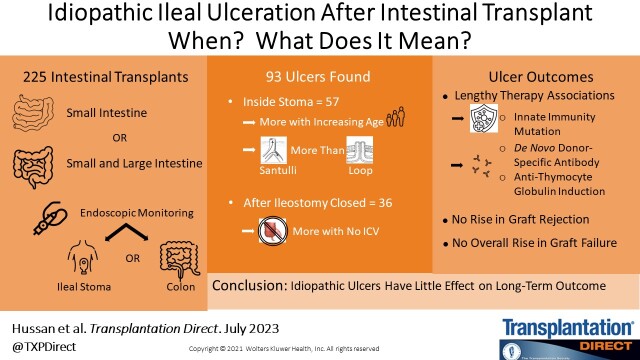
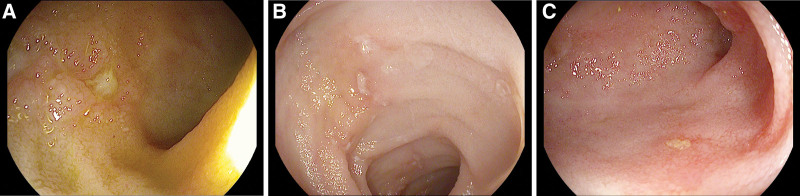
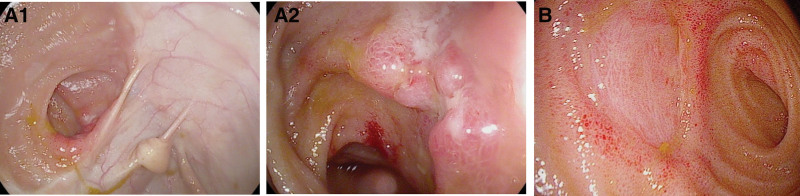
Background: Idiopathic ileal ulceration after intestinal transplantation (ITx) has been discussed infrequently and has an uncertain natural history and relation to graft rejection. Herein, we review our experience with this pathology.
Methods: We retrospectively reviewed 225 ITx in 217 patients with minimum 1 y graft survival. Routine graft endoscopy was conducted up to twice weekly within the first 90 d after ITx, gradually decreasing to once yearly. Risks for ulceration over time were evaluated using Cox regression.
Results: Of 93 (41%) patients with ulcers, 50 were found within 90 d after ITx mostly via ileoscopy; delayed healing after biopsy appeared causal in the majority. Of the remaining 43 patients with ulcers found >90 d after ITx, 36 were after ileostomy closure. Multivariable modeling demonstrated within 90-d ulcer associations with increasing patient age (hazard ratio [HR], 1.027; P < 0.001) and loop ileostomy (versus Santulli ileostomy; HR, 0.271; P < 0.001). For ulcers appearing after ileostomy closure, their sole association was with absence of graft colon (HR, 7.232; P < 0.001). For ulcers requiring extended anti-microbial and anti-inflammatory therapy, associations included de novo donor-specific antibodies (HR, 3.222; P < 0.007) and nucleotide oligomerization domain mutations (HR, 2.772; P < 0.016). Whole-cohort post-ITx ulceration was not associated with either graft rejection (P = 0.161) or graft failure (P = 0.410).
Conclusions: Idiopathic ulceration after ITx is relatively common but has little independent influence on outcome; risks include ileostomy construction, colon-free ITx, immunologic mutation, and donor sensitization.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


