S Mattke, A Gustavsson, L Jacobs, S Kern, S Palmqvist, M Eriksdotter, I Skoog, B Winblad, A Wimo, L Jönsson
{"title":"Estimates of Current Capacity for Diagnosing Alzheimer's Disease in Sweden and the Need to Expand Specialist Numbers.","authors":"S Mattke, A Gustavsson, L Jacobs, S Kern, S Palmqvist, M Eriksdotter, I Skoog, B Winblad, A Wimo, L Jönsson","doi":"10.14283/jpad.2023.94","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The emergence of disease-modifying Alzheimer's (AD) treatments provides new hope to patients and families but concerns have been raised about the preparedness of healthcare systems to provide timely access to such treatments because of a combination of a complex diagnostic process and a large prevalent pool.</p><p><strong>Objectives: </strong>We assess the preparedness of Sweden, a high-income country known for its dementia-friendly policies, to diagnose AD patients eligible for treatment within a six-month window, given current capacity for specialist evaluations and biomarker testing. We calculate the investment requirements for Sweden to achieve this target over a timeframe of 20 years.</p><p><strong>Design: </strong>Desk research to identify data for population, mortality, disease burden, cost of services and current capacity, expert consultation to inform assumptions about patient journey, and use of a Markov model to predict waiting times. The model simulates the patients' journey through different evaluation stages: initial evaluation by a primary care specialist, neurocognitive testing by an AD specialist, and confirmatory biomarker testing with PET scanning or cerebrospinal fluid (CSF) testing. The model assumes specialist appointments and PET scans are capacity constrained, and patients progress from cognitively normal to MCI and from MCI to dementia in the resulting waiting times.</p><p><strong>Measurements: </strong>Projected waiting times for diagnosis of eligibility for disease-modifying Alzheimer's treatment from 2023 to 2042 assuming current capacity, assuming 20% of Swedish residents aged 60 years and above would seek an evaluation for cognitive decline. Investments required to scale capacity up to reach target of providing diagnosis within six months on average.</p><p><strong>Results: </strong>Initial average waiting times for AD specialist appointments would be around 21 months in 2023 and remain around 55 months through 2042, as demand would continue to outstrip supply throughout the 20-year model horizon. Waiting times for biomarker testing would be stable at less than four weeks, as patients would be held up in the queue for their first specialist consultations, and use of CSF testing is widely accepted in Sweden. An additional 25% of AD specialists would have to be added above the current growth trend to reduce waiting times to less than 6 months at an average annual cost of approximately 805 million SEK. The increased cost of volume of biomarker testing would amount to about 106 million SEK per year.</p><p><strong>Conclusions: </strong>At current capacity, the Swedish healthcare system is unable to provide timely diagnosis of patients eligible for disease-modifying AD treatment. Although future diagnostic technologies, such as digital cognitive assessments and blood tests for the AD pathology, might decrease demand for capacity-constrained services, substantial investments will be required to meet a target of less than six months of waiting time for a diagnosis.</p>","PeriodicalId":48606,"journal":{"name":"Jpad-Journal of Prevention of Alzheimers Disease","volume":"1 1","pages":"155-161"},"PeriodicalIF":7.8000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10995070/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Jpad-Journal of Prevention of Alzheimers Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14283/jpad.2023.94","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The emergence of disease-modifying Alzheimer's (AD) treatments provides new hope to patients and families but concerns have been raised about the preparedness of healthcare systems to provide timely access to such treatments because of a combination of a complex diagnostic process and a large prevalent pool.
Objectives: We assess the preparedness of Sweden, a high-income country known for its dementia-friendly policies, to diagnose AD patients eligible for treatment within a six-month window, given current capacity for specialist evaluations and biomarker testing. We calculate the investment requirements for Sweden to achieve this target over a timeframe of 20 years.
Design: Desk research to identify data for population, mortality, disease burden, cost of services and current capacity, expert consultation to inform assumptions about patient journey, and use of a Markov model to predict waiting times. The model simulates the patients' journey through different evaluation stages: initial evaluation by a primary care specialist, neurocognitive testing by an AD specialist, and confirmatory biomarker testing with PET scanning or cerebrospinal fluid (CSF) testing. The model assumes specialist appointments and PET scans are capacity constrained, and patients progress from cognitively normal to MCI and from MCI to dementia in the resulting waiting times.
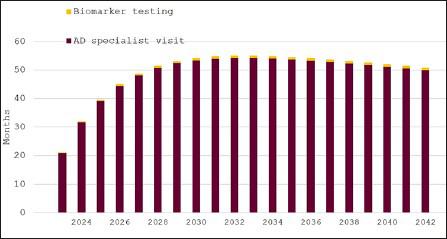
Measurements: Projected waiting times for diagnosis of eligibility for disease-modifying Alzheimer's treatment from 2023 to 2042 assuming current capacity, assuming 20% of Swedish residents aged 60 years and above would seek an evaluation for cognitive decline. Investments required to scale capacity up to reach target of providing diagnosis within six months on average.
Results: Initial average waiting times for AD specialist appointments would be around 21 months in 2023 and remain around 55 months through 2042, as demand would continue to outstrip supply throughout the 20-year model horizon. Waiting times for biomarker testing would be stable at less than four weeks, as patients would be held up in the queue for their first specialist consultations, and use of CSF testing is widely accepted in Sweden. An additional 25% of AD specialists would have to be added above the current growth trend to reduce waiting times to less than 6 months at an average annual cost of approximately 805 million SEK. The increased cost of volume of biomarker testing would amount to about 106 million SEK per year.
Conclusions: At current capacity, the Swedish healthcare system is unable to provide timely diagnosis of patients eligible for disease-modifying AD treatment. Although future diagnostic technologies, such as digital cognitive assessments and blood tests for the AD pathology, might decrease demand for capacity-constrained services, substantial investments will be required to meet a target of less than six months of waiting time for a diagnosis.
期刊介绍:
The JPAD « Journal of Prevention of Alzheimer’Disease » will publish reviews, original research articles and short reports to improve our knowledge in the field of Alzheimer prevention including : neurosciences, biomarkers, imaging, epidemiology, public health, physical cognitive exercise, nutrition, risk and protective factors, drug development, trials design, and heath economic outcomes.
JPAD will publish also the meeting abstracts from Clinical Trial on Alzheimer Disease (CTAD) and will be distributed both in paper and online version worldwide.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


