{"title":"Lessons in dialysis, dialyzers, and dialysate","authors":"Robert Hootkins MD, PhD","doi":"10.1002/dat.20609","DOIUrl":null,"url":null,"abstract":"<p>Hemodialysis today has evolved into a highly technical treatment in which knowledge of the physics and chemistry of the dialysis treatment system as well as knowledge of individual patient's pathology allows for a better understanding of how the treatment is best performed and individually modified. The “treatment prescription” is a set of specific treatment parameters that includes the treatment duration and frequency, the choice of dialyzer, and the specifics of the dialysate composition. It is imperative that the nephrologist understand how to deliver the most optimal treatment that is additionally the most cost effective.</p><p>In short, hemodialysis is the process by which a patient's blood can be chemically modified by driving it through a device (dialyzer) that allows for the removal of substances (blood solutes) as well as the gain of substances (dialysate solutes) with the additional option of the simultaneous removal of plasma water. It has evolved for almost a century but remains dependent on the chemical properties of a semipermeable membrane that is selective to the movement of solute and resistive to the movement of solvent. The primary purpose of dialysis is to eliminate uremic poisons in patients with end-stage renal disease and to modify serum electrolytes so as to mimic the appropriate serum composition of healthy individuals.</p><p>A dialyzer can be classified based on properties of the chemical composition of its membrane or based on its properties of solute removal (most commonly urea removal) and solvent permeability (most commonly water, termed <i>hydraulic permeability</i>) under specific operating conditions (blood flow rate [QB in mL/min] and dialysate flow rate [QD in mL/min]). Some dialyzers are more efficient at solute removal and are termed <i>high-efficiency</i>, whereas other dialyzers have lesser resistance to water movement and are termed <i>high-flux</i>. Dialyzer membrane properties have been recently reviewed.<span>1</span></p><p>in which the dialyzer's ability to remove a solute K is proportional to the product of the mass transfer coefficient of that dialyzer's membrane (Ko) and the membrane surface area (A). KoA is specific to a particular solute (such as urea) and is independent of QB and QD (assumption of the model). The KoA of a particular dialyzer is provided by the manufacturer, is determined in vitro in aqueous solutions, and usually overestimates by about 20% when compared with in vivo blood-based solutions containing proteins and red blood cells.</p><p>It is difficult to fully appreciate the relationships among KoA, QB, and QD. Figure 1 presents these relationships graphically, depicting urea clearance K as a function of QB for a dialyzer KoA of 1,000 and three separate QDs of 1,000, 500, and 400 mL/min (from the top curve down).</p><p>At lower QBs, the clearance (K) is linear with QD, but as QB increases closer to QD, there is a diminishing benefit of increasing QB further (as QD becomes clearance limiting).</p><p>Many insights can be obtained by an analysis of the clearance equation. Table I illustrates the effects on the overall clearance of urea of changing a number of parameters.</p><p>The first observation is that the overall clearance is simply determined by the lowest of the three parameters KoA, QB, and QD. Most high-efficiency, high-flux dialyzers have a KoA for urea of 1,000–2,000. Since QDs are typically in the range of 600–800 mL/min Dialyzer membrane properties have it is the lowest parameter, QB (typically in the range of 400–500 mL/min) that determines the overall clearance K. In fact, the more general observation is that clearance becomes limited as QB approaches either QD or KoA. Additionally, if the magnitude of both QD and KoA are close to QB, QB is even further diminished.</p><p>There are practical ramifications of these observations. One lesson is that in this current era of bundling and small financial margins, it makes sense not to spend resources on dialyzers that have excessively high KoAs in that their benefit will be minimized by the QB, which is, in turn, limited by access flow and needle resistance limitations. In general, KoAs in excess of 1,000 are of marginal benefit. An additional lesson is that with daily hemodialysis methodologies that have reduced QDs of 150 mL/min (for example, NxStage) or continuous veno-venous hemodialysis (CVVHD) techniques with QDs of 50–100 mL/min, there is no reason to employ higher QBs or to use large dialyzers, as K will be limited by QD.</p><p>Another example of an even greater waste of financial resources is the use of two dialyzers simultaneously, combined either <i>in-parallel</i> (Figure 2<i>A</i>) or <i>in-series</i> (Figure 2<i>B</i>) to effectively increase KoA.</p><p>Table II illustrates the overall effect on clearance by use of these configurations.</p><p>Although a theoretical added clearance of about 14–15% can be achieved, the total dialysis treatment “dose” can often be obtained more cost effectively by simply extending the dialysis treatment time using a single dialyzer by an additional 15–30 minutes with a minimal added cost of dialysate consumption! To employ the other configurations, additional connectors must also be purchased, increasing the costs associated with the treatment. Additionally, these configurations also result in greater dialysis disequilibrium (faster rate of solute removal, which is proportional to K/V); depending on the methodology of the urea kinetic modeling utilized, this can lead to greater overestimation of solute removal and a false sense of security that enough dialysis is being performed.</p><p>The sigma (σ) relates to the permeability of the dialysis membrane to a particular solute. This equation is the equation of a straight line, and if one experimentally measures the clearance of a molecule as a function of ultrafiltration rate, QF in mL/min, the σ and KoA can be determined from the slope (1 − σ)and the intercept (KoA).<span>3</span> Doing this for the clearance of vancomycin (molecular weight of 1,486) for a specific dialyzer (Fresenius F80) results in the determination of σ of 0.9 and a KoA of 20. Graphing the clearance (here defined as D′) of vancomycin as a function of QB and QF (Figure 3) demonstrates that it is removed more effectively with lower QBs and higher QFs.</p><p>For larger solutes cleared by convection, the greater the time of the dialysis membrane exposure (slower QB) and the greater the pressure gradient across the dialyzer membrane (higher QF), the greater the clearance. The opposite of this is true as well. For example, to minimize vancomycin clearance, faster QBs and smaller QFs will clear less of the antibiotic for a given dialysis prescription.</p><p>As a result of dialysis being performed in a in-parallel fashion, there is the generation of both an access recirculation (AR) and a cardiopulmonary recirculation (CPR). The dialyzer operating in-parallel with the peripheral access results in AR, and the peripheral access operating in-parallel with the systemic venous circulation results in CPR (Figure 4).</p><p>AR and CPR effectively prevent the dialyzer from actually receiving blood with systemic concentrations of solute; instead, a “diluted” sampling of systemic venous blood with solute cleared blood is received (Figure 5). (The extraction efficiency of a dialyzer is proportional to the incident concentration of the solute to be removed). The mathematics of these effects has been worked out by Schneditz et al.<span>4</span> As a consequence, the actual removal of solute is not only based on the dialysis treatment prescription but is also dependent on patient specific parameters that include cardiac output and venous flow through the peripheral access.</p><p>Another barrier to our effectively eliminating urea from a patient's body results from the fact that the storage of urea occurs primarily in the skeletal muscle and its removal may depend on the vascular “communication” of this compartment with the central venous system.</p><p>This provides one theory of why exercise during dialysis improves the quality of urea removal: it allows for greater vascular flow (improved communication) with the skeletal compartment and a subsequent higher central venous concentration of urea. Table III illustrates a comparison between two patients with an identical extracorporeal dialysis treatment prescription but different cardiac output and access flows.</p><p>Patient A is relatively healthy with a normal cardiac output and no significant access pathology. Patient B has mild anemia, a cardiomyopathy, and poorly functioning access flow. Ultimately, patient B receives 30% less dialysis in spite of having the same identical treatment prescription. The lesson here is that the actual delivered amount of dialysis can be significantly less than the theoretically prescribed dialysis. Flow recirculations (AR and CPR) and a patient's individual physiology (urea trapping in skeletal muscle and cardiac output) and access health result in a delivered clearance dependent on factors out of our prescriptive control. Careful consideration of a patient's cardiac status and access health may indicate a need for additional clearance beyond that predicted by an a simple analysis of his or her urea kinetic modeling.</p><p>Dialysis machines employ a proportioning system that mixes an acid concentrate with a bicarbonate concentrate and purified water. This allows for the generation of a dialysate with a physiologic pH and minimizes the possibility of forming a precipitate between bicarbonate containing alkaline solutions and calcium. The acid concentrate contains dextrose and is the source of electrolytes including potassium, calcium, magnesium, and acetic (or citric) acid. The bicarbonate concentrate may contain sodium chloride as well as sodium bicarbonate (36.83 × ) or may contain only sodium bicarbonate (35 × /45 × ). The nomenclature of the commonly used Fresenius 45x system is derived from the fact that the proportioning system mixes 1 part acid concentrate to 1.72 parts bicarbonate concentrate to 42.28 parts water, which adds up to 45 “parts.” It is important to understand that modifying the prescription for sodium or bicarbonate in real time during rounding will alter all electrolyte concentrations of the dialysate solution. Most current equipment will show the effects of changing the dialysate proportioning in real time.</p><p>It is also of importance that the total buffer in this system include bicarbonate as well as acetate (or citrate), which can add an additional 2.0–8.0 mEq/L buffer. If one prescribes a dialysate bicarbonate delivery of 35 mEq/L, the total delivered buffer will be the sum of the bicarbonate and the acetate (or citrate) from the acid concentrate (which is metabolized to bicarbonate in the liver). Therefore, the total delivered base (TDB) to a patient has to include consideration of both bicarbonate and acetate (or citrate) buffers. Consequently, on longer dialysis treatments using high bicarbonate concentrations (40 mEq/L), we can induce a chronic metabolic alkalosis, which can have adverse effects on patient mortality (based on mortality data obtained by several large dialysis providers).</p><p>One assumes that if the hemodialysis machine is set appropriately with the correct concentrates, then the dialysate composition delivered to each dialyzer is exactly as prescribed. Unfortunately, a number of variables can affect the proportioning system, one being the inlet pressure of the dialysis concentrates and water entering into the dialysis machine. Depending on the open or closed loop nature of the distribution system, inlet pressures to the machines can significantly vary even by position within the loop. To promote a more consistent pressure, a gravity feed system is often utilized. Perhaps one of the most significant aspects of the quality assessment of each dialysis facility is to ensure the correct dialysate delivery to each patient's dialyzer by sampling dialysate at the first and last chair of each distribution loop. Most dialysis specialty labs can measure electrolytes on non-blood samples and provide this as a safety check.</p>","PeriodicalId":51012,"journal":{"name":"Dialysis & Transplantation","volume":"40 9","pages":"392-396"},"PeriodicalIF":0.0000,"publicationDate":"2011-09-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1002/dat.20609","citationCount":"5","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Dialysis & Transplantation","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/dat.20609","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 5
Abstract
Hemodialysis today has evolved into a highly technical treatment in which knowledge of the physics and chemistry of the dialysis treatment system as well as knowledge of individual patient's pathology allows for a better understanding of how the treatment is best performed and individually modified. The “treatment prescription” is a set of specific treatment parameters that includes the treatment duration and frequency, the choice of dialyzer, and the specifics of the dialysate composition. It is imperative that the nephrologist understand how to deliver the most optimal treatment that is additionally the most cost effective.
In short, hemodialysis is the process by which a patient's blood can be chemically modified by driving it through a device (dialyzer) that allows for the removal of substances (blood solutes) as well as the gain of substances (dialysate solutes) with the additional option of the simultaneous removal of plasma water. It has evolved for almost a century but remains dependent on the chemical properties of a semipermeable membrane that is selective to the movement of solute and resistive to the movement of solvent. The primary purpose of dialysis is to eliminate uremic poisons in patients with end-stage renal disease and to modify serum electrolytes so as to mimic the appropriate serum composition of healthy individuals.
A dialyzer can be classified based on properties of the chemical composition of its membrane or based on its properties of solute removal (most commonly urea removal) and solvent permeability (most commonly water, termed hydraulic permeability) under specific operating conditions (blood flow rate [QB in mL/min] and dialysate flow rate [QD in mL/min]). Some dialyzers are more efficient at solute removal and are termed high-efficiency, whereas other dialyzers have lesser resistance to water movement and are termed high-flux. Dialyzer membrane properties have been recently reviewed.1
in which the dialyzer's ability to remove a solute K is proportional to the product of the mass transfer coefficient of that dialyzer's membrane (Ko) and the membrane surface area (A). KoA is specific to a particular solute (such as urea) and is independent of QB and QD (assumption of the model). The KoA of a particular dialyzer is provided by the manufacturer, is determined in vitro in aqueous solutions, and usually overestimates by about 20% when compared with in vivo blood-based solutions containing proteins and red blood cells.
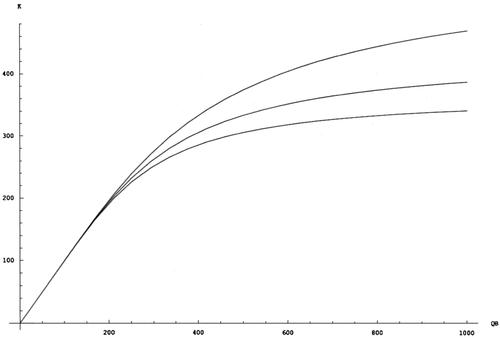
It is difficult to fully appreciate the relationships among KoA, QB, and QD. Figure 1 presents these relationships graphically, depicting urea clearance K as a function of QB for a dialyzer KoA of 1,000 and three separate QDs of 1,000, 500, and 400 mL/min (from the top curve down).
At lower QBs, the clearance (K) is linear with QD, but as QB increases closer to QD, there is a diminishing benefit of increasing QB further (as QD becomes clearance limiting).
Many insights can be obtained by an analysis of the clearance equation. Table I illustrates the effects on the overall clearance of urea of changing a number of parameters.
The first observation is that the overall clearance is simply determined by the lowest of the three parameters KoA, QB, and QD. Most high-efficiency, high-flux dialyzers have a KoA for urea of 1,000–2,000. Since QDs are typically in the range of 600–800 mL/min Dialyzer membrane properties have it is the lowest parameter, QB (typically in the range of 400–500 mL/min) that determines the overall clearance K. In fact, the more general observation is that clearance becomes limited as QB approaches either QD or KoA. Additionally, if the magnitude of both QD and KoA are close to QB, QB is even further diminished.
There are practical ramifications of these observations. One lesson is that in this current era of bundling and small financial margins, it makes sense not to spend resources on dialyzers that have excessively high KoAs in that their benefit will be minimized by the QB, which is, in turn, limited by access flow and needle resistance limitations. In general, KoAs in excess of 1,000 are of marginal benefit. An additional lesson is that with daily hemodialysis methodologies that have reduced QDs of 150 mL/min (for example, NxStage) or continuous veno-venous hemodialysis (CVVHD) techniques with QDs of 50–100 mL/min, there is no reason to employ higher QBs or to use large dialyzers, as K will be limited by QD.
Another example of an even greater waste of financial resources is the use of two dialyzers simultaneously, combined either in-parallel (Figure 2A) or in-series (Figure 2B) to effectively increase KoA.
Table II illustrates the overall effect on clearance by use of these configurations.
Although a theoretical added clearance of about 14–15% can be achieved, the total dialysis treatment “dose” can often be obtained more cost effectively by simply extending the dialysis treatment time using a single dialyzer by an additional 15–30 minutes with a minimal added cost of dialysate consumption! To employ the other configurations, additional connectors must also be purchased, increasing the costs associated with the treatment. Additionally, these configurations also result in greater dialysis disequilibrium (faster rate of solute removal, which is proportional to K/V); depending on the methodology of the urea kinetic modeling utilized, this can lead to greater overestimation of solute removal and a false sense of security that enough dialysis is being performed.
The sigma (σ) relates to the permeability of the dialysis membrane to a particular solute. This equation is the equation of a straight line, and if one experimentally measures the clearance of a molecule as a function of ultrafiltration rate, QF in mL/min, the σ and KoA can be determined from the slope (1 − σ)and the intercept (KoA).3 Doing this for the clearance of vancomycin (molecular weight of 1,486) for a specific dialyzer (Fresenius F80) results in the determination of σ of 0.9 and a KoA of 20. Graphing the clearance (here defined as D′) of vancomycin as a function of QB and QF (Figure 3) demonstrates that it is removed more effectively with lower QBs and higher QFs.
For larger solutes cleared by convection, the greater the time of the dialysis membrane exposure (slower QB) and the greater the pressure gradient across the dialyzer membrane (higher QF), the greater the clearance. The opposite of this is true as well. For example, to minimize vancomycin clearance, faster QBs and smaller QFs will clear less of the antibiotic for a given dialysis prescription.
As a result of dialysis being performed in a in-parallel fashion, there is the generation of both an access recirculation (AR) and a cardiopulmonary recirculation (CPR). The dialyzer operating in-parallel with the peripheral access results in AR, and the peripheral access operating in-parallel with the systemic venous circulation results in CPR (Figure 4).
AR and CPR effectively prevent the dialyzer from actually receiving blood with systemic concentrations of solute; instead, a “diluted” sampling of systemic venous blood with solute cleared blood is received (Figure 5). (The extraction efficiency of a dialyzer is proportional to the incident concentration of the solute to be removed). The mathematics of these effects has been worked out by Schneditz et al.4 As a consequence, the actual removal of solute is not only based on the dialysis treatment prescription but is also dependent on patient specific parameters that include cardiac output and venous flow through the peripheral access.
Another barrier to our effectively eliminating urea from a patient's body results from the fact that the storage of urea occurs primarily in the skeletal muscle and its removal may depend on the vascular “communication” of this compartment with the central venous system.
This provides one theory of why exercise during dialysis improves the quality of urea removal: it allows for greater vascular flow (improved communication) with the skeletal compartment and a subsequent higher central venous concentration of urea. Table III illustrates a comparison between two patients with an identical extracorporeal dialysis treatment prescription but different cardiac output and access flows.
Patient A is relatively healthy with a normal cardiac output and no significant access pathology. Patient B has mild anemia, a cardiomyopathy, and poorly functioning access flow. Ultimately, patient B receives 30% less dialysis in spite of having the same identical treatment prescription. The lesson here is that the actual delivered amount of dialysis can be significantly less than the theoretically prescribed dialysis. Flow recirculations (AR and CPR) and a patient's individual physiology (urea trapping in skeletal muscle and cardiac output) and access health result in a delivered clearance dependent on factors out of our prescriptive control. Careful consideration of a patient's cardiac status and access health may indicate a need for additional clearance beyond that predicted by an a simple analysis of his or her urea kinetic modeling.
Dialysis machines employ a proportioning system that mixes an acid concentrate with a bicarbonate concentrate and purified water. This allows for the generation of a dialysate with a physiologic pH and minimizes the possibility of forming a precipitate between bicarbonate containing alkaline solutions and calcium. The acid concentrate contains dextrose and is the source of electrolytes including potassium, calcium, magnesium, and acetic (or citric) acid. The bicarbonate concentrate may contain sodium chloride as well as sodium bicarbonate (36.83 × ) or may contain only sodium bicarbonate (35 × /45 × ). The nomenclature of the commonly used Fresenius 45x system is derived from the fact that the proportioning system mixes 1 part acid concentrate to 1.72 parts bicarbonate concentrate to 42.28 parts water, which adds up to 45 “parts.” It is important to understand that modifying the prescription for sodium or bicarbonate in real time during rounding will alter all electrolyte concentrations of the dialysate solution. Most current equipment will show the effects of changing the dialysate proportioning in real time.
It is also of importance that the total buffer in this system include bicarbonate as well as acetate (or citrate), which can add an additional 2.0–8.0 mEq/L buffer. If one prescribes a dialysate bicarbonate delivery of 35 mEq/L, the total delivered buffer will be the sum of the bicarbonate and the acetate (or citrate) from the acid concentrate (which is metabolized to bicarbonate in the liver). Therefore, the total delivered base (TDB) to a patient has to include consideration of both bicarbonate and acetate (or citrate) buffers. Consequently, on longer dialysis treatments using high bicarbonate concentrations (40 mEq/L), we can induce a chronic metabolic alkalosis, which can have adverse effects on patient mortality (based on mortality data obtained by several large dialysis providers).
One assumes that if the hemodialysis machine is set appropriately with the correct concentrates, then the dialysate composition delivered to each dialyzer is exactly as prescribed. Unfortunately, a number of variables can affect the proportioning system, one being the inlet pressure of the dialysis concentrates and water entering into the dialysis machine. Depending on the open or closed loop nature of the distribution system, inlet pressures to the machines can significantly vary even by position within the loop. To promote a more consistent pressure, a gravity feed system is often utilized. Perhaps one of the most significant aspects of the quality assessment of each dialysis facility is to ensure the correct dialysate delivery to each patient's dialyzer by sampling dialysate at the first and last chair of each distribution loop. Most dialysis specialty labs can measure electrolytes on non-blood samples and provide this as a safety check.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


