Systemic azithromycin versus amoxicillin/metronidazole as an adjunct in the treatment of periodontitis: a systematic review and meta-analysis
Abstract
Background
The use of systemic azithromycin (AZT) and amoxicillin/metronidazole (AMX/MTZ) as adjuncts provided additional clinical and microbiological benefits over subgingival instrumentation alone. However, the superiority of one antibiotic regimen over another has not been proven. Therefore, the aim of this systematic review and meta-analyses was to evaluate the clinical efficacy and safety of subgingival instrumentation (SI) in conjunction with the systemic use of AZT or AMX/MTZ for the treatment of periodontitis from current published literature.
Methods
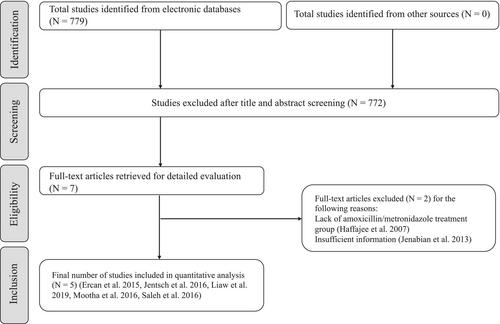
Electronic databases were searched to identify randomized controlled trials (RCTs), controlled clinical trials, prospective and retrospective human studies that compared the adjunctive use of systemic AZT to AMX/MTZ with SI in the treatment of periodontitis. The eligibility criteria were defined based on the participant (who had periodontitis), intervention (SI with adjunctive use of systemic AZT), comparison (SI with adjunctive use of systemic AMX/MTZ), outcomes (primary outcome: changes in probing pocket). The risk of bias was assessed using the Cochrane Collaboration's Risk of Bias tool. Data were analysed using a statistical software program.
Results
Five studies with 151 participants with periodontitis were included in the present review. Of these, 74 participants received adjunctive AZT, while the remaining participants received AMX/MTZ as an adjunct to SI. The adjunctive use of AZT and AMX/MTZ had comparable changes in probing pocket depths at 1–3 months with no statistically significant difference (mean difference (MD) 0.01; 95% CI –0.20 to 0.22; P = 0.94). The adjunctive use of AZT had significantly fewer number of residual sites with probing pocket depths of ≥5 mm at 1–3 months compared to the adjunctive use of AMX/MTZ (MD –3.41; 95% CI –4.73 to –2.10; P < 0.0001). The prevalence rates of adverse events among participants who received AZT and AMX/MTZ were 9.80% and 14.8%, respectively. The meta-analysis showed that the difference between the two groups was not statistically significant (risk ratio 0.69; 95% CI 0.28 to 1.72; P = 0.43).
Conclusions
Within the limitation of this review, there was no superiority between AZT and AMX/MTZ in terms of mean changes in probing pocket depths, clinical attachment level, bleeding on probing at 1–3 months. AZT seem to be associated with less sites with residual probing pocket depths of ≥5 mm at 1–3 months and fewer adverse events compared with AMX/MTZ. © 2023 Australian Dental Association.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


