Nicholas Graves, Raju Maiti, Fazila Abu Bakar Aloweni, Ng Yi Zhen, Ang Shin Yuh, Priya Bishnoi, Tze Tec Chong, David Carmody, Keith Harding
{"title":"Retrospective matched cohort study of incidence rates and excess length of hospital stay owing to pressure injuries in an Asian setting","authors":"Nicholas Graves, Raju Maiti, Fazila Abu Bakar Aloweni, Ng Yi Zhen, Ang Shin Yuh, Priya Bishnoi, Tze Tec Chong, David Carmody, Keith Harding","doi":"10.1002/hcs2.30","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Little is known about stage 1 and 2 pressure injuries that are health care-acquired. We report incidence rates of health care-acquired stage 1 and stage 2 pressure injuries, and, estimate the excess length of stay using four competing analytic methods. We discuss the merits of the different approaches.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We calculated monthly incidence rates for stage 1 and 2 health care-acquired pressure injuries occurring in a large Singapore acute care hospital. To estimate excess stay, we conducted unadjusted comparisons with a control cohort, performed linear regression and then generalized linear regression with a gamma distribution. Finally, we fitted a simple state-based model. The design for the cost attribution work was a retrospective matched cohort study.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Incidence rates in 2016 were 0.553% (95% confidence interval [CI] 0.55, 0.557) and 0.469% (95% CI 0.466, 0.472) in 2017. For data censored at 60 days’ maximum stay, the unadjusted comparisons showed the highest excess stay at 17.68 (16.43-18.93) days and multi-state models showed the lowest at 1.22 (0.19, 2.23) days.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Poor-quality methods for attribution of excess length of stay to pressure injury generate inflated estimates that could mislead decision makers. The findings from the multi-state model, which is an appropriate method, are plausible and illustrate the likely bed-days saved from lowering the risk of these events. Stage 1 and 2 pressure injuries are common and increase costs by prolonging the length of stay. There will be economic value investing in prevention. Using biased estimates of excess length of stay will overstate the potential value of prevention.</p>\n </section>\n </div>","PeriodicalId":100601,"journal":{"name":"Health Care Science","volume":"2 2","pages":"82-93"},"PeriodicalIF":0.0000,"publicationDate":"2023-03-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hcs2.30","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Care Science","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hcs2.30","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Little is known about stage 1 and 2 pressure injuries that are health care-acquired. We report incidence rates of health care-acquired stage 1 and stage 2 pressure injuries, and, estimate the excess length of stay using four competing analytic methods. We discuss the merits of the different approaches.
Methods
We calculated monthly incidence rates for stage 1 and 2 health care-acquired pressure injuries occurring in a large Singapore acute care hospital. To estimate excess stay, we conducted unadjusted comparisons with a control cohort, performed linear regression and then generalized linear regression with a gamma distribution. Finally, we fitted a simple state-based model. The design for the cost attribution work was a retrospective matched cohort study.
Results
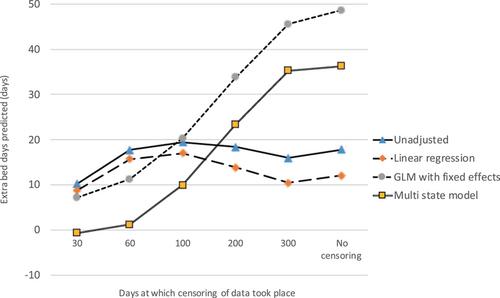
Incidence rates in 2016 were 0.553% (95% confidence interval [CI] 0.55, 0.557) and 0.469% (95% CI 0.466, 0.472) in 2017. For data censored at 60 days’ maximum stay, the unadjusted comparisons showed the highest excess stay at 17.68 (16.43-18.93) days and multi-state models showed the lowest at 1.22 (0.19, 2.23) days.
Conclusions
Poor-quality methods for attribution of excess length of stay to pressure injury generate inflated estimates that could mislead decision makers. The findings from the multi-state model, which is an appropriate method, are plausible and illustrate the likely bed-days saved from lowering the risk of these events. Stage 1 and 2 pressure injuries are common and increase costs by prolonging the length of stay. There will be economic value investing in prevention. Using biased estimates of excess length of stay will overstate the potential value of prevention.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


