Gastric Peroral Endoscopic Myotomy as a Therapeutic Option in Refractory Gastroparesis: A Step-By-Step Description.
IF 1
Q4 GASTROENTEROLOGY & HEPATOLOGY
GE Portuguese Journal of Gastroenterology
Pub Date : 2022-11-03
eCollection Date: 2023-10-01
DOI:10.1159/000527016
引用次数: 0
Abstract
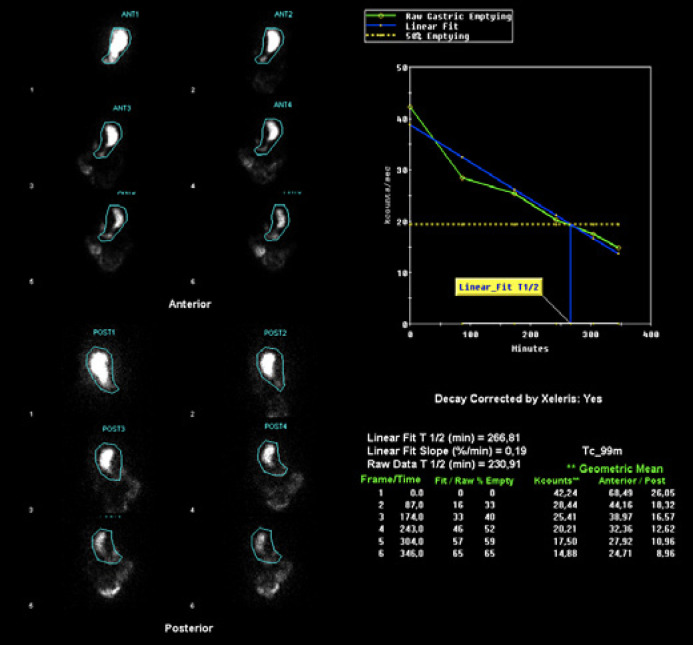
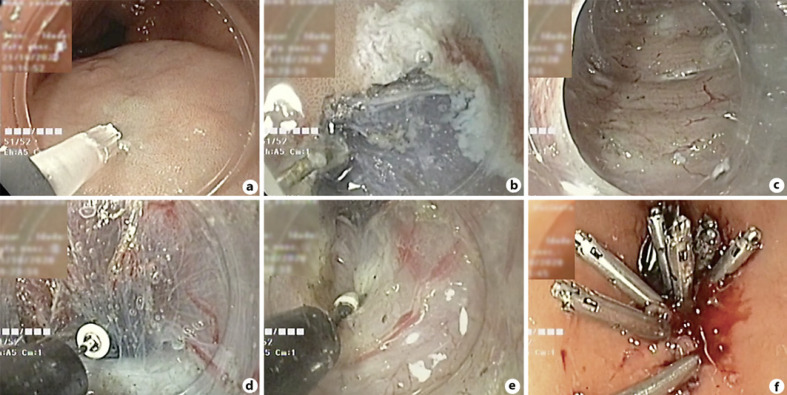
Gastroparesis is a chronic disorder characterized by delayed gastric emptying without evidence of stomach or proximal small intestine obstruction [1]. Its pathophysiology is unclear, although gastric arrhythmias, fundal and antral hypocontractility, pylorospasm, and antropyloroduodenal incoordination might be involved [1]. Dietary modifications and prokinetics are first-line treatments. When refractory gastroparesis is present, surgical or endoscopic treatment must be considered. We present a case of a 68-year-old female patient, followed in gastroenterology consult due to nausea, persistent postprandial vomiting, early satiety, and belching. She has no relevant past medical or surgical history or medication. Esophagogastroduodenoscopy revealed food stasis but was otherwise normal. Gastric emptying scintigraphy (GES) showed emptying of 30% at 156 min, 46% at 217 min, and 54% at 260 min, with significant radiopharmaceutical retention (46% at 4 h 18 min), translating scintigraphic evidence of delayed gastric emptying (Fig. 1). The diagnosis of gastroparesis was made, and medical therapy was optimized. She had no improvement after 6 months, traducing a Gastroparesis Cardinal Symptom Index (GCSI) score of 3.33 points (0–5 points) [2]. Idiopathic refractory gastroparesis was admitted, and gastric peroral endoscopic myotomy (G-POEM) was proposed. The procedure was performed with an endoscope (GIF-HQ190; Olympus Medical Systems, Tokyo, Japan), with a transparent distal cap (DH28GR; Fujifilm, Tokyo, Japan) and insufflation with CO2. The patient was under general anesthesia and orotracheal intubation. The VIO®3 (Erbe Elektromedizin GmbH, Tuebingen, Germany) was used as the electrosurgical unit. Antibiotic (cefotaxime 1 g) was administered. The procedure began with submucosal injection, in the greater gastric curvature, 5 cm proximal to the pylorus with a solution of 100
胃经口内镜下肌切开术作为难治性胃轻瘫的治疗选择:分步描述。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

GE Portuguese Journal of Gastroenterology
GASTROENTEROLOGY & HEPATOLOGY-
CiteScore
1.60
自引率
11.10%
发文量
62
审稿时长
21 weeks
期刊介绍:
The ''GE Portuguese Journal of Gastroenterology'' (formerly Jornal Português de Gastrenterologia), founded in 1994, is the official publication of Sociedade Portuguesa de Gastrenterologia (Portuguese Society of Gastroenterology), Sociedade Portuguesa de Endoscopia Digestiva (Portuguese Society of Digestive Endoscopy) and Associação Portuguesa para o Estudo do Fígado (Portuguese Association for the Study of the Liver). The journal publishes clinical and basic research articles on Gastroenterology, Digestive Endoscopy, Hepatology and related topics. Review articles, clinical case studies, images, letters to the editor and other articles such as recommendations or papers on gastroenterology clinical practice are also considered. Only articles written in English are accepted.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


