{"title":"A case of extensive alopecia areata following Pfizer-BioNTech BNT162b2 mRNA COVID-19 vaccine with favorable outcome","authors":"Yoshihiro Matsuda MD, Yoshio Kawakami MD, PhD, Masaya Kawamoto MD, Yoji Hirai MD, PhD, Shin Morizane MD, PhD","doi":"10.1002/cia2.12292","DOIUrl":null,"url":null,"abstract":"<p>The coronavirus disease 2019 (COVID-19) pandemic has an enormous impact on dermatological practice. There are many articles describing COVID-19-related and COVID-19 vaccine-related hair loss, such as telogen effluvium (TE), alopecia areata (AA), friction alopecia and anagen effluvium,<span><sup>1</sup></span> although their clinical outcomes have been poorly documented. We report a case of extensive AA following administration of the Pfzer-BioNTech BNT162b2 mRNA COVID-19 vaccine with favorable outcome.</p><p>A 37-year-old woman with no significant medical history except for childhood atopic dermatitis, developed persistent low-grade fever (37.2°C) on day +13 after the first dose of BNT162b2 mRNA vaccine (all date numbers refer to the first dose). Subsequently, the patient noticed coin-sized hair loss on day +22, and it became widespread within 1 week. Laboratory examinations performed at a nearby clinic on day +31 showed increased serum C-reactive protein (3.53 mg/dl) and decreased white blood cells (3000/μl) with 54.0% of neutrophils, 2.4% of eosinophils, and 34.8% of lymphocytes, whereas serological tests for syphilis were negative, and serum thyroid function tests, antinuclear antibody, immunoglobulin E, and thymus activation-regulated chemokine levels were all within normal ranges. She received the second dose BNT162b2 mRNA vaccine on day +32. The persistent low-grade fever spontaneously resolved on day +34 although the hair loss continued to aggravate. She presented to our hospital on day +73 for further evaluation. Physical examination revealed widespread alopecia with a severity of alopecia tool (SALT) II score of 80 (Figure 1A), whereas her eyebrows, eyelashes, and body hair were intact. Trichoscopy showed tapering hairs, broken hairs, black dots, and increase in vacant follicular ostia (Figure 1B). Histological findings of a skin biopsy revealed perifollicular lymphocytic infiltrate and increased number of telogen hairs (Figure 1C–E). Results of direct immunofluorescence studies were negative. We treated the patient with topical betamethasone butyrate propionate lotion. On day +120, the patient showed a sign of hair regrowth. The patient's hair mostly recovered leaving only one oval bald patch on day +310, and SALT II score decreased to 5 (Figure 1F).</p><p>The hair loss in this patient occurred following a febrile condition after the first dose of BNT162b2 mRNA vaccine, and we initially considered the patient as TE. However, initial onset with coin-sized hair loss and the presence of an oval bald patch in the late phase were rather characteristic for AA.</p><p>A review of the literature including the present case identified 17 cases of AA associated with COVID-19 vaccines.<span><sup>2-7</sup></span> Six cases had a previous history of AA. Types of vaccines prior to the development of AA included BNT162b2 mRNA in 11 cases, AZD1222/ChAdOx1 viral vector in three cases, and mRNA-1273 in three cases. In eight cases, AA appeared after the first dose, and four of them displayed aggravation of AA following the second dose. Their precise clinical outcomes were not documented, except for one case showing areas of sparse regrowth,<span><sup>6</sup></span> Our case displayed recovery of hair growth with topical corticosteroid therapy, suggesting that some cases of COVID-19 vaccine-related AA might recover without aggressive treatment.</p><p>The authors declare no conflicts of interest.</p><p>Approval of the research protocol: No human participant was involved in this study.</p><p>Informed consent: N/A.</p><p>Registry and the registration no. of the study/trial: N/A.</p><p>Animal Studies: N/A.</p>","PeriodicalId":15543,"journal":{"name":"Journal of Cutaneous Immunology and Allergy","volume":"6 3","pages":"115-116"},"PeriodicalIF":1.1000,"publicationDate":"2023-01-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cia2.12292","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cutaneous Immunology and Allergy","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cia2.12292","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"ALLERGY","Score":null,"Total":0}
引用次数: 0
Abstract
The coronavirus disease 2019 (COVID-19) pandemic has an enormous impact on dermatological practice. There are many articles describing COVID-19-related and COVID-19 vaccine-related hair loss, such as telogen effluvium (TE), alopecia areata (AA), friction alopecia and anagen effluvium,1 although their clinical outcomes have been poorly documented. We report a case of extensive AA following administration of the Pfzer-BioNTech BNT162b2 mRNA COVID-19 vaccine with favorable outcome.
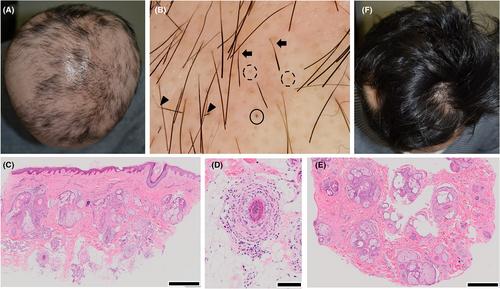
A 37-year-old woman with no significant medical history except for childhood atopic dermatitis, developed persistent low-grade fever (37.2°C) on day +13 after the first dose of BNT162b2 mRNA vaccine (all date numbers refer to the first dose). Subsequently, the patient noticed coin-sized hair loss on day +22, and it became widespread within 1 week. Laboratory examinations performed at a nearby clinic on day +31 showed increased serum C-reactive protein (3.53 mg/dl) and decreased white blood cells (3000/μl) with 54.0% of neutrophils, 2.4% of eosinophils, and 34.8% of lymphocytes, whereas serological tests for syphilis were negative, and serum thyroid function tests, antinuclear antibody, immunoglobulin E, and thymus activation-regulated chemokine levels were all within normal ranges. She received the second dose BNT162b2 mRNA vaccine on day +32. The persistent low-grade fever spontaneously resolved on day +34 although the hair loss continued to aggravate. She presented to our hospital on day +73 for further evaluation. Physical examination revealed widespread alopecia with a severity of alopecia tool (SALT) II score of 80 (Figure 1A), whereas her eyebrows, eyelashes, and body hair were intact. Trichoscopy showed tapering hairs, broken hairs, black dots, and increase in vacant follicular ostia (Figure 1B). Histological findings of a skin biopsy revealed perifollicular lymphocytic infiltrate and increased number of telogen hairs (Figure 1C–E). Results of direct immunofluorescence studies were negative. We treated the patient with topical betamethasone butyrate propionate lotion. On day +120, the patient showed a sign of hair regrowth. The patient's hair mostly recovered leaving only one oval bald patch on day +310, and SALT II score decreased to 5 (Figure 1F).
The hair loss in this patient occurred following a febrile condition after the first dose of BNT162b2 mRNA vaccine, and we initially considered the patient as TE. However, initial onset with coin-sized hair loss and the presence of an oval bald patch in the late phase were rather characteristic for AA.
A review of the literature including the present case identified 17 cases of AA associated with COVID-19 vaccines.2-7 Six cases had a previous history of AA. Types of vaccines prior to the development of AA included BNT162b2 mRNA in 11 cases, AZD1222/ChAdOx1 viral vector in three cases, and mRNA-1273 in three cases. In eight cases, AA appeared after the first dose, and four of them displayed aggravation of AA following the second dose. Their precise clinical outcomes were not documented, except for one case showing areas of sparse regrowth,6 Our case displayed recovery of hair growth with topical corticosteroid therapy, suggesting that some cases of COVID-19 vaccine-related AA might recover without aggressive treatment.
The authors declare no conflicts of interest.
Approval of the research protocol: No human participant was involved in this study.
Informed consent: N/A.
Registry and the registration no. of the study/trial: N/A.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


