{"title":"Earlier continuous administration of mepolizumab for eosinophilic granulomatosis with polyangiitis based on cutaneous findings","authors":"Takaharu Ikeda MD, PhD, Toshiro Komatsu MD, Kae Yokoyama MD, Tamihiro Kawakami MD, PhD","doi":"10.1002/cia2.12295","DOIUrl":null,"url":null,"abstract":"<p>Treatment of eosinophilic granulomatosis with polyangiitis (EGPA) remains a challenge because currently available therapies, corticosteroids, and immunomodulators, do not always control symptoms and are often associated with significant morbidity and relapse. We previously proposed that the initial cutaneous clinical and histopathologic findings based on skin biopsy and peripheral blood findings, as hallmark manifestations of EGPA, could prompt dermatologists to consider this diagnosis at an earlier stage.<span><sup>1</sup></span> Based on these cutaneous findings, we also reported that earlier adjunct administration of mepolizumab and intravenous immunoglobulin therapy (IVIG) led to significant improvement in EGPA symptoms.<span><sup>2</sup></span> Since those initial reports, we have been able to maintain good control of the disease, allowing us to taper their prednisolone dosage without any negative impact on the improvement of these symptoms or any significant adverse effects related to the drugs during a 3-year follow-up.</p><p>A 55-year-old man presented with erythematous nodules and livedo racemosa with purpura on his leg edema. There were clinical signs of mononeuritis multiplex as evidence of peripheral neurologic involvement. Microscopic examination of the indurated nodules revealed necrotizing vasculitis in the lower dermis and subcutaneous fat. There was a predominance of eosinophil infiltration into the dermis around the vascular walls and nerve fiber. He had been treated with oral prednisolone and intravenous cyclophosphamide pulse therapy (IVCY). The therapy did not resolve his symptoms, including the associated multiple mononeuritis. We administered IVIG, 400 mg/kg for 5 days, and mepolizumab 300 mg subcutaneously every 4 weeks to address concerns of exacerbation of complications such as peripheral neuropathy. The symptoms gradually improved, with resolution of the peripheral eosinophilia and normalized IgE levels. Azathioprine was additionally administered from the 6th month as prednisolone was tapered smoothly. To date, he has not developed any additional vasculitis symptoms during the 3-year follow-up (Figure 1A).</p><p>A 30-year-old woman presented with slightly purpuric skin lesions on her lower extremities. Nerve conduction tests revealed a mononeuritis multiplex on her lower extremities. Microscopic examination of skin biopsy specimens obtained from the purpura revealed leukocytoclastic vasculitis. There was a predominance of eosinophils infiltrating the dermis around the nerve fiber. We applied an adjunct combination therapy of IVIG and mepolizumab. After two courses of this adjunct therapy, the cutaneous manifestations, as well as the arthritis and mononeuritis multiplex had been completely resolved along with the normalization of peripheral eosinophilia, without any remarkable adverse effects related to prednisone such as opportunistic infections. Prednisolone was subsequently tapered smoothly. After 3 years, there has been no evidence of clinical recurrence or adverse effects of the systemic corticosteroids (Figure 1B).</p><p>The most important objective in the treatment of EGPA is to induce long-term remission and reduce the burden of systemic glucocorticoids and immunosuppressive therapies. Some studies have reported on the ability of mepolizumab to induce remission, prevent relapses, and allow a reduction in glucocorticoid dose.<span><sup>3-5</sup></span> We propose that earlier continuous administration of mepolizumab could be useful in controlling relapse and refractory disease, and can reduce the need for less desirable treatment protocols such as long-term corticosteroids.</p><p>The authors declare no conflict of interest.</p><p>Approval of the research protocol: Yes. N/A?</p><p>Informed Consent: Yes.</p><p>Registry and the Registration No.: N/A.</p><p>Animal Studies: N/A.</p>","PeriodicalId":15543,"journal":{"name":"Journal of Cutaneous Immunology and Allergy","volume":"6 4","pages":"132-133"},"PeriodicalIF":0.9000,"publicationDate":"2023-01-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cia2.12295","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cutaneous Immunology and Allergy","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cia2.12295","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"ALLERGY","Score":null,"Total":0}
引用次数: 0
Abstract
Treatment of eosinophilic granulomatosis with polyangiitis (EGPA) remains a challenge because currently available therapies, corticosteroids, and immunomodulators, do not always control symptoms and are often associated with significant morbidity and relapse. We previously proposed that the initial cutaneous clinical and histopathologic findings based on skin biopsy and peripheral blood findings, as hallmark manifestations of EGPA, could prompt dermatologists to consider this diagnosis at an earlier stage.1 Based on these cutaneous findings, we also reported that earlier adjunct administration of mepolizumab and intravenous immunoglobulin therapy (IVIG) led to significant improvement in EGPA symptoms.2 Since those initial reports, we have been able to maintain good control of the disease, allowing us to taper their prednisolone dosage without any negative impact on the improvement of these symptoms or any significant adverse effects related to the drugs during a 3-year follow-up.
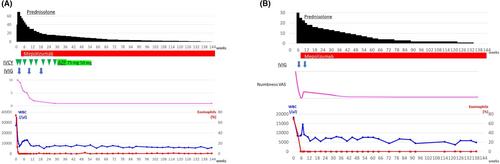
A 55-year-old man presented with erythematous nodules and livedo racemosa with purpura on his leg edema. There were clinical signs of mononeuritis multiplex as evidence of peripheral neurologic involvement. Microscopic examination of the indurated nodules revealed necrotizing vasculitis in the lower dermis and subcutaneous fat. There was a predominance of eosinophil infiltration into the dermis around the vascular walls and nerve fiber. He had been treated with oral prednisolone and intravenous cyclophosphamide pulse therapy (IVCY). The therapy did not resolve his symptoms, including the associated multiple mononeuritis. We administered IVIG, 400 mg/kg for 5 days, and mepolizumab 300 mg subcutaneously every 4 weeks to address concerns of exacerbation of complications such as peripheral neuropathy. The symptoms gradually improved, with resolution of the peripheral eosinophilia and normalized IgE levels. Azathioprine was additionally administered from the 6th month as prednisolone was tapered smoothly. To date, he has not developed any additional vasculitis symptoms during the 3-year follow-up (Figure 1A).
A 30-year-old woman presented with slightly purpuric skin lesions on her lower extremities. Nerve conduction tests revealed a mononeuritis multiplex on her lower extremities. Microscopic examination of skin biopsy specimens obtained from the purpura revealed leukocytoclastic vasculitis. There was a predominance of eosinophils infiltrating the dermis around the nerve fiber. We applied an adjunct combination therapy of IVIG and mepolizumab. After two courses of this adjunct therapy, the cutaneous manifestations, as well as the arthritis and mononeuritis multiplex had been completely resolved along with the normalization of peripheral eosinophilia, without any remarkable adverse effects related to prednisone such as opportunistic infections. Prednisolone was subsequently tapered smoothly. After 3 years, there has been no evidence of clinical recurrence or adverse effects of the systemic corticosteroids (Figure 1B).
The most important objective in the treatment of EGPA is to induce long-term remission and reduce the burden of systemic glucocorticoids and immunosuppressive therapies. Some studies have reported on the ability of mepolizumab to induce remission, prevent relapses, and allow a reduction in glucocorticoid dose.3-5 We propose that earlier continuous administration of mepolizumab could be useful in controlling relapse and refractory disease, and can reduce the need for less desirable treatment protocols such as long-term corticosteroids.
治疗嗜酸性肉芽肿病合并多血管炎(EGPA)仍然是一个挑战,因为目前可用的治疗方法,皮质类固醇和免疫调节剂,并不总能控制症状,往往与显著的发病率和复发有关。我们之前提出,基于皮肤活检和外周血结果的最初皮肤临床和组织病理学发现,作为EGPA的标志性表现,可以促使皮肤科医生在早期阶段考虑这种诊断基于这些皮肤发现,我们也报道了早期辅助给予mepolizumab和静脉免疫球蛋白治疗(IVIG)可显著改善EGPA症状自这些初步报告以来,我们已经能够保持对疾病的良好控制,使我们能够逐渐减少泼尼松龙的剂量,而不会对这些症状的改善产生任何负面影响,也不会在3年的随访中出现与药物相关的任何重大不良反应。一个55岁的男人提出了红斑结节和活的总状斑紫癜在他的腿水肿。多发性单神经炎的临床表现为周围神经受累的证据。显微镜检查硬化结节显示坏死性血管炎在下真皮和皮下脂肪。血管壁及神经纤维周围真皮以嗜酸性细胞浸润为主。他接受口服强的松龙和静脉环磷酰胺脉冲治疗(IVCY)。治疗没有解决他的症状,包括相关的多发性单神经炎。我们给予IVIG, 400mg /kg,持续5天,mepolizumab每4周皮下注射300mg,以解决并发症恶化的问题,如周围神经病变。随着外周血嗜酸性粒细胞增多和IgE水平正常化,症状逐渐改善。从第6个月开始,随着泼尼松龙逐渐逐渐减少,我们开始额外使用硫唑嘌呤。到目前为止,在3年的随访中,他没有出现任何额外的血管炎症状(图1A)。一名30岁女性下肢出现轻微紫癜性皮肤病变。神经传导测试显示她的下肢有多发性单神经炎紫癜患者皮肤活检标本的显微检查显示白细胞分裂性血管炎。神经纤维周围真皮以嗜酸性粒细胞浸润为主。我们采用了IVIG和mepolizumab的辅助联合治疗。经过两个疗程的辅助治疗,皮肤表现以及关节炎和多发性单神经炎已完全消失,周围嗜酸性粒细胞正常化,未出现与强的松相关的明显不良反应,如机会性感染。强的松龙随后逐渐逐渐减少。3年后,没有临床复发或全身性皮质类固醇不良反应的证据(图1B)。EGPA治疗的最重要目标是诱导长期缓解,减轻全身糖皮质激素和免疫抑制治疗的负担。一些研究报道了mepolizumab诱导缓解、预防复发和减少糖皮质激素剂量的能力。3-5我们建议早期持续给予mepolizumab可能有助于控制复发和难治性疾病,并可以减少对不太理想的治疗方案(如长期皮质类固醇)的需求。作者声明无利益冲突。研究方案的批准:是的。N / A ?知情同意:是的。注册处及注册编号: N / A。动物研究:无。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


