Eva Leidman, Muhammad Ali Jatoi, Iris Bollemeijer, Jennifer Majer, Shannon Doocy
{"title":"Accuracy of Fully Automated 3D Imaging System for Child Anthropometry in a Low-Resource Setting: Effectiveness Evaluation in Malakal, South Sudan.","authors":"Eva Leidman, Muhammad Ali Jatoi, Iris Bollemeijer, Jennifer Majer, Shannon Doocy","doi":"10.2196/40066","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Adoption of 3D imaging systems in humanitarian settings requires accuracy comparable with manual measurement notwithstanding additional constraints associated with austere settings.</p><p><strong>Objective: </strong>This study aimed to evaluate the accuracy of child stature and mid-upper arm circumference (MUAC) measurements produced by the AutoAnthro 3D imaging system (third generation) developed by Body Surface Translations Inc.</p><p><strong>Methods: </strong>A study of device accuracy was embedded within a 2-stage cluster survey at the Malakal Protection of Civilians site in South Sudan conducted between September 2021 and October 2021. All children aged 6 to 59 months within selected households were eligible. For each child, manual measurements were obtained by 2 anthropometrists following the protocol used in the 2006 World Health Organization Child Growth Standards study. Scans were then captured by a different enumerator using a Samsung Galaxy 8 phone loaded with a custom software, AutoAnthro, and an Intel RealSense 3D scanner. The scans were processed using a fully automated algorithm. A multivariate logistic regression model was fit to evaluate the adjusted odds of achieving a successful scan. The accuracy of the measurements was visually assessed using Bland-Altman plots and quantified using average bias, limits of agreement (LoAs), and the 95% precision interval for individual differences. Key informant interviews were conducted remotely with survey enumerators and Body Surface Translations Inc developers to understand challenges in beta testing, training, data acquisition and transmission.</p><p><strong>Results: </strong>Manual measurements were obtained for 539 eligible children, and scan-derived measurements were successfully processed for 234 (43.4%) of them. Caregivers of at least 10.4% (56/539) of the children refused consent for scan capture; additional scans were unsuccessfully transmitted to the server. Neither the demographic characteristics of the children (age and sex), stature, nor MUAC were associated with availability of scan-derived measurements; team was significantly associated (P<.001). The average bias of scan-derived measurements in cm was -0.5 (95% CI -2.0 to 1.0) for stature and 0.7 (95% CI 0.4-1.0) for MUAC. For stature, the 95% LoA was -23.9 cm to 22.9 cm. For MUAC, the 95% LoA was -4.0 cm to 5.4 cm. All accuracy metrics varied considerably by team. The COVID-19 pandemic-related physical distancing and travel policies limited testing to validate the device algorithm and prevented developers from conducting in-person training and field oversight, negatively affecting the quality of scan capture, processing, and transmission.</p><p><strong>Conclusions: </strong>Scan-derived measurements were not sufficiently accurate for the widespread adoption of the current technology. Although the software shows promise, further investments in the software algorithms are needed to address issues with scan transmission and extreme field contexts as well as to enable improved field supervision. Differences in accuracy by team provide evidence that investment in training may also improve performance.</p>","PeriodicalId":87288,"journal":{"name":"JMIR biomedical engineering","volume":" ","pages":"e40066"},"PeriodicalIF":0.0000,"publicationDate":"2022-10-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11041446/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR biomedical engineering","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/40066","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Adoption of 3D imaging systems in humanitarian settings requires accuracy comparable with manual measurement notwithstanding additional constraints associated with austere settings.
Objective: This study aimed to evaluate the accuracy of child stature and mid-upper arm circumference (MUAC) measurements produced by the AutoAnthro 3D imaging system (third generation) developed by Body Surface Translations Inc.
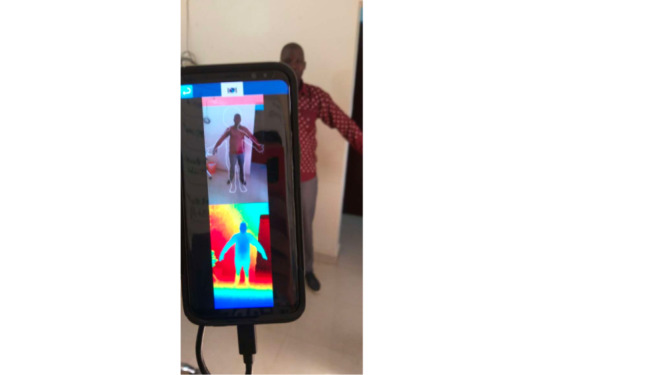
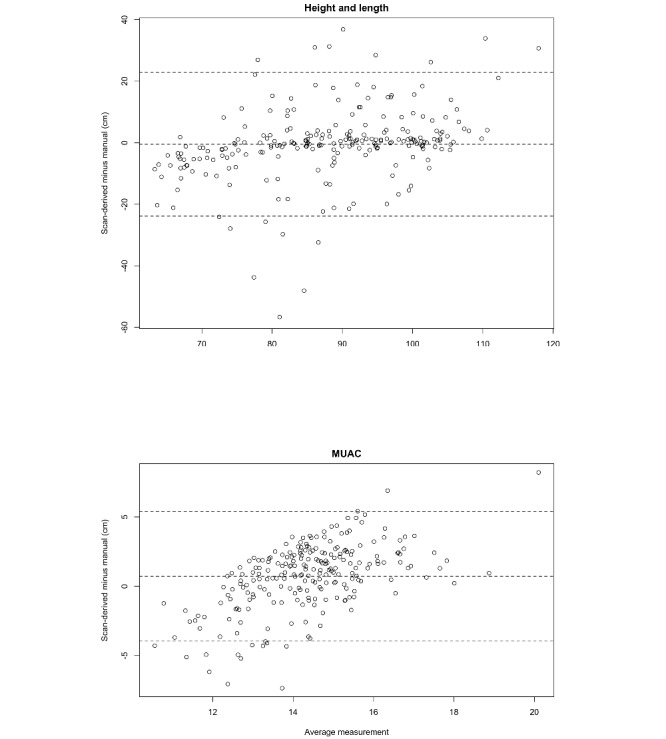
Methods: A study of device accuracy was embedded within a 2-stage cluster survey at the Malakal Protection of Civilians site in South Sudan conducted between September 2021 and October 2021. All children aged 6 to 59 months within selected households were eligible. For each child, manual measurements were obtained by 2 anthropometrists following the protocol used in the 2006 World Health Organization Child Growth Standards study. Scans were then captured by a different enumerator using a Samsung Galaxy 8 phone loaded with a custom software, AutoAnthro, and an Intel RealSense 3D scanner. The scans were processed using a fully automated algorithm. A multivariate logistic regression model was fit to evaluate the adjusted odds of achieving a successful scan. The accuracy of the measurements was visually assessed using Bland-Altman plots and quantified using average bias, limits of agreement (LoAs), and the 95% precision interval for individual differences. Key informant interviews were conducted remotely with survey enumerators and Body Surface Translations Inc developers to understand challenges in beta testing, training, data acquisition and transmission.
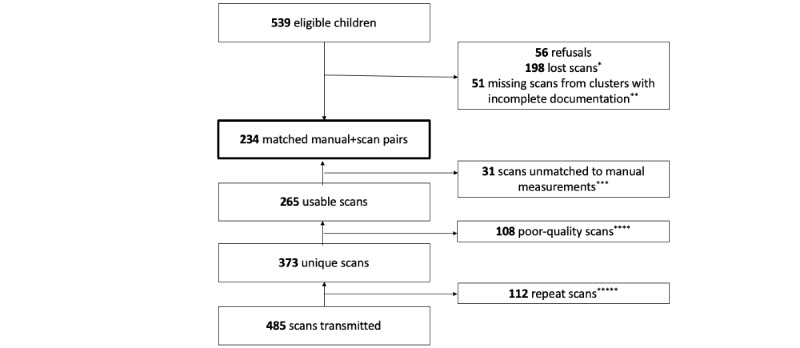
Results: Manual measurements were obtained for 539 eligible children, and scan-derived measurements were successfully processed for 234 (43.4%) of them. Caregivers of at least 10.4% (56/539) of the children refused consent for scan capture; additional scans were unsuccessfully transmitted to the server. Neither the demographic characteristics of the children (age and sex), stature, nor MUAC were associated with availability of scan-derived measurements; team was significantly associated (P<.001). The average bias of scan-derived measurements in cm was -0.5 (95% CI -2.0 to 1.0) for stature and 0.7 (95% CI 0.4-1.0) for MUAC. For stature, the 95% LoA was -23.9 cm to 22.9 cm. For MUAC, the 95% LoA was -4.0 cm to 5.4 cm. All accuracy metrics varied considerably by team. The COVID-19 pandemic-related physical distancing and travel policies limited testing to validate the device algorithm and prevented developers from conducting in-person training and field oversight, negatively affecting the quality of scan capture, processing, and transmission.
Conclusions: Scan-derived measurements were not sufficiently accurate for the widespread adoption of the current technology. Although the software shows promise, further investments in the software algorithms are needed to address issues with scan transmission and extreme field contexts as well as to enable improved field supervision. Differences in accuracy by team provide evidence that investment in training may also improve performance.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


