{"title":"Erythema annulare centrifugum in the setting of COVID-19 infection: A case report and literature review","authors":"Misako Fujisaki MD, Takumi Hasegawa MD, Noritaka Oyama MD, PhD, Koji Yamaoka MD, Masaki Anzai MD, PhD, Minoru Hasegawa MD, PhD","doi":"10.1002/cia2.12274","DOIUrl":null,"url":null,"abstract":"<p>Erythema annulare centrifugum (EAC) is a figurate papulo-erythema following a self-limiting course, caused by a variety of underlying factors. Skin manifestations associated with COVID-19 infection considerably vary,<span><sup>1</sup></span> and sometimes exhibit clinically ambiguous appearance compared to the original disease image (e.g., erythema multiforme-like, Gianotti-Crosti-like, pernio-like, and livedo-like eruptions),<span><sup>2-5</sup></span> but COVID-19-associated EAC or similar eruption has rarely been reported to date.</p><p>An otherwise healthy 49-year-old Japanese male who had a 2-week history of malaise was diagnosed with COVID-19 by a positive reverse transcription-polymerase chain reaction for SARS-CoV-2. He had never received the SARS-CoV-2 vaccine. The next day after receiving 200 mg/day of remdesivir intravenously, asymptomatic erythema appeared suddenly on the lumbar and extremities. Physical examination showed non-coalescent edematous erythema with partially defined borders on the lumbar and legs (Figure 1A,B). A routine laboratory test and screening for autoimmune diseases showed no abnormal findings, except for atypical lymphocytes and elevated CRP. The chest CT showed diffuse frosted shadows in both lungs suggestive of COVID-19. Skin biopsy revealed focal spongiosis, vacuolar changes along with the dermo-epidermal junction, and densely packed inflammatory cell infiltrates around blood vessels in the superficial dermis (Figure 1C). The infiltrating cells are composed of predominant lymphocytes and scant eosinophils with a “coat-sleeve”-like appearance (Figure 1D). The clinicopathological findings raised the diagnosis of EAC. After discontinuation of remdesivir, he was treated with topical steroids and oral antihistamine, providing successful remission of the skin lesion by 1 month, as the COVID-19-related symptoms lessened. The skin lesion has never recurred thereafter.</p><p>Most cases with EAC are clinically idiopathic, although the current concept regarding the disease pathogenesis suggests a delayed-type hypersensitivity to various antigens, including viral, bacterial, or fungal infections, drugs, foods, malignancy or other systemic diseases.<span><sup>6</sup></span> This is supported by evidence that the skin manifestation of EAC is alleviated by treatment of the underlying disease. EAC associated with viral infection has been reported to be triggered by various viruses, such as EB virus, poxvirus, HIV, varicella-zoster virus, and influenza virus, and is mostly transient like our case or displays a fluctuating skin lesion in parallel with the viral disease activity.</p><p>To our knowledge, there have been only four case reports, including ours, for EAC encountered in association with COVID-19 infection; one of whom resolved with oral doxycycline,<span><sup>7</sup></span> and three others improved with topical steroids and/or antihistamine.<span><sup>8, 9</sup></span> Except one child case,<span><sup>8</sup></span> their skin lesions appeared about 1 week after the onset of COVID-19 infection and disappeared within 1 month, suggesting the consequence of viral infection itself and/or preceded antiviral therapy. Except our case, however, the remaining three cases have received neither antiviral therapy including remdesivir nor any of drugs. COVID-19 infection may cause impaired immune response with dysregulation of proinflammatory cytokines, particularly tumor necrosis factor-α,<span><sup>10</sup></span> thus implicating the underlying immunopathogenic similarity between COVID-19 infection and EAC. EAC associated with COVID-19, therefore, remains presumptive further awaiting similar case series to update evidence for the pathogenesis and response to treatment, and also proper recognition of dermatologists.</p><p>\n <span>The authors declare no conflict of interest.</span>\n </p><p>Approval of the research protocol: No human participant was involved in this study.</p><p>Informed consent: N/A.</p><p>Registry and the Registration No. of the study/trial: N/A.</p><p>Animal <span>Studies</span>: N/A.</p>","PeriodicalId":15543,"journal":{"name":"Journal of Cutaneous Immunology and Allergy","volume":"6 2","pages":"57-58"},"PeriodicalIF":0.9000,"publicationDate":"2022-08-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cia2.12274","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cutaneous Immunology and Allergy","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cia2.12274","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"ALLERGY","Score":null,"Total":0}
引用次数: 0
Abstract
Erythema annulare centrifugum (EAC) is a figurate papulo-erythema following a self-limiting course, caused by a variety of underlying factors. Skin manifestations associated with COVID-19 infection considerably vary,1 and sometimes exhibit clinically ambiguous appearance compared to the original disease image (e.g., erythema multiforme-like, Gianotti-Crosti-like, pernio-like, and livedo-like eruptions),2-5 but COVID-19-associated EAC or similar eruption has rarely been reported to date.
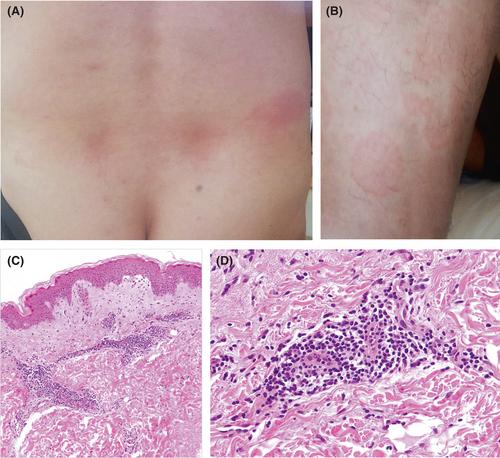
An otherwise healthy 49-year-old Japanese male who had a 2-week history of malaise was diagnosed with COVID-19 by a positive reverse transcription-polymerase chain reaction for SARS-CoV-2. He had never received the SARS-CoV-2 vaccine. The next day after receiving 200 mg/day of remdesivir intravenously, asymptomatic erythema appeared suddenly on the lumbar and extremities. Physical examination showed non-coalescent edematous erythema with partially defined borders on the lumbar and legs (Figure 1A,B). A routine laboratory test and screening for autoimmune diseases showed no abnormal findings, except for atypical lymphocytes and elevated CRP. The chest CT showed diffuse frosted shadows in both lungs suggestive of COVID-19. Skin biopsy revealed focal spongiosis, vacuolar changes along with the dermo-epidermal junction, and densely packed inflammatory cell infiltrates around blood vessels in the superficial dermis (Figure 1C). The infiltrating cells are composed of predominant lymphocytes and scant eosinophils with a “coat-sleeve”-like appearance (Figure 1D). The clinicopathological findings raised the diagnosis of EAC. After discontinuation of remdesivir, he was treated with topical steroids and oral antihistamine, providing successful remission of the skin lesion by 1 month, as the COVID-19-related symptoms lessened. The skin lesion has never recurred thereafter.
Most cases with EAC are clinically idiopathic, although the current concept regarding the disease pathogenesis suggests a delayed-type hypersensitivity to various antigens, including viral, bacterial, or fungal infections, drugs, foods, malignancy or other systemic diseases.6 This is supported by evidence that the skin manifestation of EAC is alleviated by treatment of the underlying disease. EAC associated with viral infection has been reported to be triggered by various viruses, such as EB virus, poxvirus, HIV, varicella-zoster virus, and influenza virus, and is mostly transient like our case or displays a fluctuating skin lesion in parallel with the viral disease activity.
To our knowledge, there have been only four case reports, including ours, for EAC encountered in association with COVID-19 infection; one of whom resolved with oral doxycycline,7 and three others improved with topical steroids and/or antihistamine.8, 9 Except one child case,8 their skin lesions appeared about 1 week after the onset of COVID-19 infection and disappeared within 1 month, suggesting the consequence of viral infection itself and/or preceded antiviral therapy. Except our case, however, the remaining three cases have received neither antiviral therapy including remdesivir nor any of drugs. COVID-19 infection may cause impaired immune response with dysregulation of proinflammatory cytokines, particularly tumor necrosis factor-α,10 thus implicating the underlying immunopathogenic similarity between COVID-19 infection and EAC. EAC associated with COVID-19, therefore, remains presumptive further awaiting similar case series to update evidence for the pathogenesis and response to treatment, and also proper recognition of dermatologists.
The authors declare no conflict of interest.
Approval of the research protocol: No human participant was involved in this study.
Informed consent: N/A.
Registry and the Registration No. of the study/trial: N/A.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


