{"title":"Hydroxyzine-induced fixed drug eruption and cross-reaction with oxatomide","authors":"Mizuki Terada MD, Shujiro Hayashi MD, PhD, Maki Okamoto MD, Ken Igawa MD, PhD","doi":"10.1002/cia2.12275","DOIUrl":null,"url":null,"abstract":"<p>Oxatomide and hydroxyzine are two anti-H1 antihistamines used for treating urticaria, pruritus dermatitis, pollinosis, and several other diseases. In general, anti-H1 antihistamines rarely elicit cutaneous adverse effects.<span><sup>1</sup></span> We report a case of fixed drug eruption (FDE) caused by the cross-reaction between oxatomide and hydroxyzine.</p><p>A 50-year-old woman had a history of taking oxatomide for seasonal pollinosis. She took oxatomide in the first season of 2002. Painful erythema and erosions appeared 5 h after taking the drug. These symptoms appeared on the lower lip and at the mucocutaneous junction (Figure 1A), with positive results in the patch test (PT; Figure 1B) for oxatomide and oral challenge test. The same skin lesion appeared 5 h after taking oxatomide; these results led to the diagnosis of oxatomide-induced FDE. This eruption improved after the discontinuation of oxatomide and administration of prednisolone (PSL) at 0.6 mg/kg/day for 1 week.</p><p>We previously reported and published the above-mentioned case until this clinical point.<span><sup>2</sup></span> Although she took eszopiclone and bepotastine besilate for insomnia because of pollinosis, no drug eruption appeared. One year later, she took hydroxyzine for the first time for sleeplessness because of pollinosis. On the next morning, she had fever and subsequently experienced lip discomfort. Furthermore, on the next day, erythema, blisters, and erosions appeared around the lower lip (Figure 1C). These eruptions were almost similar to the previously described oxatomide-induced FDE. PT against hydroxyzine revealed positive results, and the patient was diagnosed with hydroxyzine-induced FDE (Figure 1D). The eruptions improved using the same treatment that was used for oxatomide-induced eruptions. Moreover, pollinosis-associated insomnia improved using eszopiclone and did not cause any skin eruptions.</p><p>FDE is a clinical form of drug eruption that induces erythema in the same region of the body after each administration of the causative drug. PT at the lesion is an effective means for diagnosis.<span><sup>3</sup></span> However, few reports have implicated such drugs in the development of FDE, particularly the piperazine derivatives, such as hydroxyzine, cetirizine, and levocetirizine.<span><sup>1</sup></span> Bhari et al.<span><sup>4</sup></span> reported the case of a patient with an allergy to a drug containing a piperazine ring, who presented a cross-reaction to two other drugs containing piperazine rings. There are no reports on the cross-reactivity between oxatomide and hydroxyzine; however, both share a piperazine ring structure (red circles in Figure 1E,F). Thus, cross-reactivity could appear. In this case, although eszopiclone has a piperazine ring (Figure 1G), no eruption has been reported to date. Therefore, the antigenic determinant in our case was not a piperazine ring. Oxatomide and hydroxyzine share not only a piperazine ring but also two benzene rings via a methine group (=CH–; green square in Figure 1E,F). This shared structural group was suggested to become an antigenic determinant and results in cross-reactivity. To the best of our knowledge, such a unique case has not yet been reported, and the possibility of a novel antigenic structural group associated with FDE is proposed in this case, which needs further investigations.</p><p>The authors declare no conflicts of interest.</p><p>Approval of the research protocol: No human participant was involved in this study.</p><p>Informed Consent: Informed consent was obtained from the patient.</p><p>Registry and the Registration No. of the study/trial: N/A. Animal Studies: N/A.</p>","PeriodicalId":15543,"journal":{"name":"Journal of Cutaneous Immunology and Allergy","volume":"6 2","pages":"59-60"},"PeriodicalIF":0.9000,"publicationDate":"2022-09-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cia2.12275","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cutaneous Immunology and Allergy","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cia2.12275","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"ALLERGY","Score":null,"Total":0}
引用次数: 0
Abstract
Oxatomide and hydroxyzine are two anti-H1 antihistamines used for treating urticaria, pruritus dermatitis, pollinosis, and several other diseases. In general, anti-H1 antihistamines rarely elicit cutaneous adverse effects.1 We report a case of fixed drug eruption (FDE) caused by the cross-reaction between oxatomide and hydroxyzine.
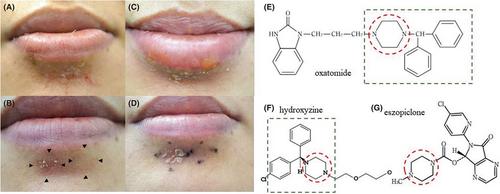
A 50-year-old woman had a history of taking oxatomide for seasonal pollinosis. She took oxatomide in the first season of 2002. Painful erythema and erosions appeared 5 h after taking the drug. These symptoms appeared on the lower lip and at the mucocutaneous junction (Figure 1A), with positive results in the patch test (PT; Figure 1B) for oxatomide and oral challenge test. The same skin lesion appeared 5 h after taking oxatomide; these results led to the diagnosis of oxatomide-induced FDE. This eruption improved after the discontinuation of oxatomide and administration of prednisolone (PSL) at 0.6 mg/kg/day for 1 week.
We previously reported and published the above-mentioned case until this clinical point.2 Although she took eszopiclone and bepotastine besilate for insomnia because of pollinosis, no drug eruption appeared. One year later, she took hydroxyzine for the first time for sleeplessness because of pollinosis. On the next morning, she had fever and subsequently experienced lip discomfort. Furthermore, on the next day, erythema, blisters, and erosions appeared around the lower lip (Figure 1C). These eruptions were almost similar to the previously described oxatomide-induced FDE. PT against hydroxyzine revealed positive results, and the patient was diagnosed with hydroxyzine-induced FDE (Figure 1D). The eruptions improved using the same treatment that was used for oxatomide-induced eruptions. Moreover, pollinosis-associated insomnia improved using eszopiclone and did not cause any skin eruptions.
FDE is a clinical form of drug eruption that induces erythema in the same region of the body after each administration of the causative drug. PT at the lesion is an effective means for diagnosis.3 However, few reports have implicated such drugs in the development of FDE, particularly the piperazine derivatives, such as hydroxyzine, cetirizine, and levocetirizine.1 Bhari et al.4 reported the case of a patient with an allergy to a drug containing a piperazine ring, who presented a cross-reaction to two other drugs containing piperazine rings. There are no reports on the cross-reactivity between oxatomide and hydroxyzine; however, both share a piperazine ring structure (red circles in Figure 1E,F). Thus, cross-reactivity could appear. In this case, although eszopiclone has a piperazine ring (Figure 1G), no eruption has been reported to date. Therefore, the antigenic determinant in our case was not a piperazine ring. Oxatomide and hydroxyzine share not only a piperazine ring but also two benzene rings via a methine group (=CH–; green square in Figure 1E,F). This shared structural group was suggested to become an antigenic determinant and results in cross-reactivity. To the best of our knowledge, such a unique case has not yet been reported, and the possibility of a novel antigenic structural group associated with FDE is proposed in this case, which needs further investigations.
The authors declare no conflicts of interest.
Approval of the research protocol: No human participant was involved in this study.
Informed Consent: Informed consent was obtained from the patient.
Registry and the Registration No. of the study/trial: N/A. Animal Studies: N/A.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


