Myeloablative haploidentical t-cell replete hematopoietic cell transplantation with post-transplant cyclophosphamide in high-risk hematological malignancies: Bending the learning curve in a middle-income setting
Sanket P. Shah, Vivek S. Radhakrishnan, Ganesh S. Jaishetwar, Reghu K. Sukumaran, Jeevan Kumar, Saurabh J. Bhave, Mita Roychowdhury, Sayak Chaudhuri, Deepak K. Mishra, Reena Nair, Shekhar Krishnan, Mammen Chandy
{"title":"Myeloablative haploidentical t-cell replete hematopoietic cell transplantation with post-transplant cyclophosphamide in high-risk hematological malignancies: Bending the learning curve in a middle-income setting","authors":"Sanket P. Shah, Vivek S. Radhakrishnan, Ganesh S. Jaishetwar, Reghu K. Sukumaran, Jeevan Kumar, Saurabh J. Bhave, Mita Roychowdhury, Sayak Chaudhuri, Deepak K. Mishra, Reena Nair, Shekhar Krishnan, Mammen Chandy","doi":"10.1002/acg2.106","DOIUrl":null,"url":null,"abstract":"<p>Haploidentical peripheral blood hematopoietic cell transplantation has become the preferred alternative donor transplant program in most centers in India, owing to its logistic and cost advantages. This is a retrospective analysis of 59 patients with high-risk hematological malignancies who underwent haploidentical transplant in three different centers, using myeloablative conditioning and unmanipulated stem cell graft. GVHD prophylaxis was post-transplant Cyclophosphamide (PTCy D + 3, D + 4) along with Tacrolimus and Mycophenolate Mofetil (D + 5 onwards). The median CD34 cell dose was 5.8 x 10<sup>6</sup> cells/kg. Neutrophils engrafted in 50 (83%) patients [median time D + 16 (range: 12-38)] and platelets engrafted in 42 patients (70%) [median time D + 17 (range: 12-50)]. Acute GVHD developed in 25 (41.7%) patients [Gr III/IV in 9] and Chronic GVHD in 15 (38.5%). 100-day mortality was 33.8%. With a median follow-up duration of 6.2 months (range: 0.4-50.8 months), the relapse rate, treatment-related mortality (TRM), and estimated 4-year overall survival are 10.0%, 43.3%, and 38.0%, respectively. For the 31 deaths: causes included engraftment failure (n = 7), GVHD (n = 7), persistent disease (n = 1), relapsed disease (n = 5), bacterial sepsis (n = 5), viral pneumonia (n = 1), infection (n = 3), secondary graft failure (n = 2). TRM outcomes have reduced over time with experience. Myeloablative conditioning and haploidentical transplantation by a post-transplant cyclophosphamide approach is feasible in a resource-constrained setting, despite higher rates of GVHD and infection-related mortality.</p>","PeriodicalId":72084,"journal":{"name":"Advances in cell and gene therapy","volume":"4 2","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2020-12-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1002/acg2.106","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in cell and gene therapy","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/acg2.106","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
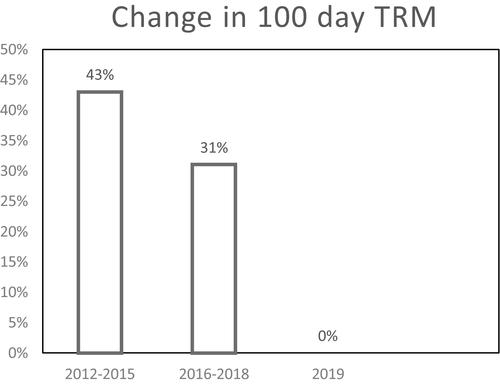
Haploidentical peripheral blood hematopoietic cell transplantation has become the preferred alternative donor transplant program in most centers in India, owing to its logistic and cost advantages. This is a retrospective analysis of 59 patients with high-risk hematological malignancies who underwent haploidentical transplant in three different centers, using myeloablative conditioning and unmanipulated stem cell graft. GVHD prophylaxis was post-transplant Cyclophosphamide (PTCy D + 3, D + 4) along with Tacrolimus and Mycophenolate Mofetil (D + 5 onwards). The median CD34 cell dose was 5.8 x 106 cells/kg. Neutrophils engrafted in 50 (83%) patients [median time D + 16 (range: 12-38)] and platelets engrafted in 42 patients (70%) [median time D + 17 (range: 12-50)]. Acute GVHD developed in 25 (41.7%) patients [Gr III/IV in 9] and Chronic GVHD in 15 (38.5%). 100-day mortality was 33.8%. With a median follow-up duration of 6.2 months (range: 0.4-50.8 months), the relapse rate, treatment-related mortality (TRM), and estimated 4-year overall survival are 10.0%, 43.3%, and 38.0%, respectively. For the 31 deaths: causes included engraftment failure (n = 7), GVHD (n = 7), persistent disease (n = 1), relapsed disease (n = 5), bacterial sepsis (n = 5), viral pneumonia (n = 1), infection (n = 3), secondary graft failure (n = 2). TRM outcomes have reduced over time with experience. Myeloablative conditioning and haploidentical transplantation by a post-transplant cyclophosphamide approach is feasible in a resource-constrained setting, despite higher rates of GVHD and infection-related mortality.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


