{"title":"Bulging and sunken major duodenal papilla","authors":"Chi-Ying Yang, Wen-Hsin Huang","doi":"10.1002/aid2.13368","DOIUrl":null,"url":null,"abstract":"<p>A 41-year-old man presented with intermittent epigastric fullness for several weeks. Mild hyperbilirubinemia was incidentally discovered when he was young, but he was not further examined. For a few weeks, the patient felt right upper quadrant (RUQ) fullness, which was exacerbated after meals. The physical examination indicated mild RUQ tenderness without Murphy's sign. Hepatitis and jaundice were noted. Computed tomography of the abdomen revealed biliary tract dilatation at the distal common bile duct (Figure 1A). Endoscopic retrograde cholangiopancreatography (ERCP) revealed a bulging lesion at the roof of the major duodenal papilla, which first protruded and then flattened and sunken (Figure 1B,C).</p><p>What is the diagnosis?</p><p>Choledochocele was diagnosed by cholangiogram (Figure 2A) and an endoscopic sphincterotomy (Figure 2B) was performed. Choledochal cyst is a rare congenital biliary cystic disease whose etiology is still unknown. The choledochocele is characterized by cystic dilatation at the pancreaticobiliary junction and protrusion to the duodenum and is subdivided into Types A and B by Sarris and Tsang in 1989.<span><sup>1</sup></span> Type A choledochocele is cystic dilatation of bile duct in ampulla and is located proximal to orifice of ampulla. Type B choledochocele is located distal to orifice of ampulla and is diverticula of common channel in ampulla. The duodenal duplication cyst was congenital malformations, which was mimic as choledochocele. Endoscopic ultrasonography or abdominal magnetic resonance cholangiopancreatography can help to distinguish duodenal duplication cyst from a choledochocele. In choledochocele, cholangiogram showed contrast medium accumulation in the bulge at the end of the common bile duct, which may not be present in a duplication cyst.<span><sup>2</sup></span> ERCP is used for the management of cholangitis, obstructive jaundice, or biliary malignancy.</p><p>Complete excision of the cyst is the standard treatment. Surgical procedures are chosen according to subtype and endoscopic sphincterotomy or transduodenal complete cyst excision is used for choledochocele management. After the choledochal cyst is removed, the remnant biliary tract may still develop a malignancy. The incidence of remaining biliary malignant transformation after cyst excision was 4.3%, and malignant tumors of the intrahepatic, hilar, or extrahepatic bile duct may occur over time.<span><sup>3</sup></span></p><p>The authors declare no conflicts of interest.</p><p>The study participant provided informed consent and this report was approved by the Institutional Review Board of China Medical University Hospital at Taichung (No. CMUH111-REC1-136).</p>","PeriodicalId":7278,"journal":{"name":"Advances in Digestive Medicine","volume":"11 2","pages":"101-102"},"PeriodicalIF":0.4000,"publicationDate":"2023-06-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/aid2.13368","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Digestive Medicine","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/aid2.13368","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
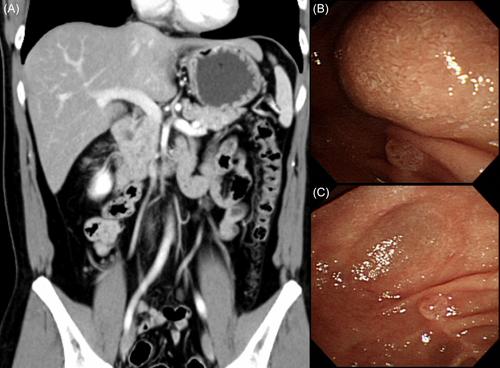
A 41-year-old man presented with intermittent epigastric fullness for several weeks. Mild hyperbilirubinemia was incidentally discovered when he was young, but he was not further examined. For a few weeks, the patient felt right upper quadrant (RUQ) fullness, which was exacerbated after meals. The physical examination indicated mild RUQ tenderness without Murphy's sign. Hepatitis and jaundice were noted. Computed tomography of the abdomen revealed biliary tract dilatation at the distal common bile duct (Figure 1A). Endoscopic retrograde cholangiopancreatography (ERCP) revealed a bulging lesion at the roof of the major duodenal papilla, which first protruded and then flattened and sunken (Figure 1B,C).
What is the diagnosis?
Choledochocele was diagnosed by cholangiogram (Figure 2A) and an endoscopic sphincterotomy (Figure 2B) was performed. Choledochal cyst is a rare congenital biliary cystic disease whose etiology is still unknown. The choledochocele is characterized by cystic dilatation at the pancreaticobiliary junction and protrusion to the duodenum and is subdivided into Types A and B by Sarris and Tsang in 1989.1 Type A choledochocele is cystic dilatation of bile duct in ampulla and is located proximal to orifice of ampulla. Type B choledochocele is located distal to orifice of ampulla and is diverticula of common channel in ampulla. The duodenal duplication cyst was congenital malformations, which was mimic as choledochocele. Endoscopic ultrasonography or abdominal magnetic resonance cholangiopancreatography can help to distinguish duodenal duplication cyst from a choledochocele. In choledochocele, cholangiogram showed contrast medium accumulation in the bulge at the end of the common bile duct, which may not be present in a duplication cyst.2 ERCP is used for the management of cholangitis, obstructive jaundice, or biliary malignancy.
Complete excision of the cyst is the standard treatment. Surgical procedures are chosen according to subtype and endoscopic sphincterotomy or transduodenal complete cyst excision is used for choledochocele management. After the choledochal cyst is removed, the remnant biliary tract may still develop a malignancy. The incidence of remaining biliary malignant transformation after cyst excision was 4.3%, and malignant tumors of the intrahepatic, hilar, or extrahepatic bile duct may occur over time.3
The authors declare no conflicts of interest.
The study participant provided informed consent and this report was approved by the Institutional Review Board of China Medical University Hospital at Taichung (No. CMUH111-REC1-136).
期刊介绍:
Advances in Digestive Medicine is the official peer-reviewed journal of GEST, DEST and TASL. Missions of AIDM are to enhance the quality of patient care, to promote researches in gastroenterology, endoscopy and hepatology related fields, and to develop platforms for digestive science. Specific areas of interest are included, but not limited to: • Acid-related disease • Small intestinal disease • Digestive cancer • Diagnostic & therapeutic endoscopy • Enteral nutrition • Innovation in endoscopic technology • Functional GI • Hepatitis • GI images • Liver cirrhosis • Gut hormone • NASH • Helicobacter pylori • Cancer screening • IBD • Laparoscopic surgery • Infectious disease of digestive tract • Genetics and metabolic disorder • Microbiota • Regenerative medicine • Pancreaticobiliary disease • Guideline & consensus.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


