Aimin Jiang, Le Qu, Bing Liu, Anbang Wang, Linhui Wang
{"title":"Reconsidering the role of receptors for SARS-CoV-2 in clear cell renal cell carcinoma: Friends or foes","authors":"Aimin Jiang, Le Qu, Bing Liu, Anbang Wang, Linhui Wang","doi":"10.1002/mef2.31","DOIUrl":null,"url":null,"abstract":"<p>At the end of 2019, the new coronavirus began to spread around the world. World Health Organization named this virus SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2), which caused coronavirus disease (COVID-19). In most people without underlying medical conditions, symptoms of SARS-CoV-2 infection are often mild and nonlethal. However, patients with cancer have significantly higher rates of severe SARS-CoV-2 infection and disease-related mortality than normal individuals.<span><sup>1</sup></span> Numerous studies have shown that progressive malignancy is an independent risk factor for severe SARS-CoV-2 infection and related death. The incidence of long-term sequelae of SARS-CoV-2 infection in cancer patients is estimated at 15%–30%.<span><sup>2</sup></span> Although the use of vaccines has reduced the chance of severe SARS-CoV-2 infection incidence, large-scale trials often exclude cancer patients. It remains to be seen how effective and safe the vaccine is in cancer patients and how long it is durable. Multiorgan single-cell sequencing analysis confirmed that key receptors for SARS-CoV-2 infection in humans include ACE2 (angiotensin-converting enzyme 2), TMPRSS2 (transmembrane serine protease 2), NRP1 (neuropilin-1), AXL (AXL receptor tyrosine kinase), FURIN, and CTSL1 (cathepsin L1).<span><sup>3</sup></span> SARS-CoV-2 infection may directly or indirectly lead to acute kidney injury, which may be related to the cytophilic effects of the virus and cytokine-induced systemic inflammatory responses. These receptors may play a key role in SARS-CoV-2 infection-induced acute kidney injury and even death. These key receptors provide crucial evidence for the development of antiviral drugs for SARS-CoV-2. However, further research on these receptors in cancer patients is warranted.</p><p>First, the expression profiling of prognosis prediction was investigated in multicancers. We found that except TMPRSS2, the remaining five receptors (ACE2, NRP1, AXL, FURIN, and CTSL1) were upregulated in various cancers, especially in kidney renal clear cell carcinoma (KIRC) (Figure 1A). The relationship between these receptors and the prognosis of cancer patients was analyzed. The results suggested that these four receptors, ACE2, NRP1, FURIN, and CTSL1, were prognostic risk factors in various cancers such as glioma, while in KIRC, they are protective factors for overall survival (Figure 1B). Similarly, ACE2, NRP1, and CTSL1 receptors were prognostic risk factors in gliomas and other tumors, and protective factors for disease progression-free survival in KIRC (Figure 1B). The protective induction of these three receptors on KIRC was also confirmed in the GSE29609 data set and the Japan-KIRC database (Figure 1C). The expression pattern of SARS-CoV-2 infection-related receptors in KIRC is different from other malignancies. ACE2, NRP1, and CTSL1 were highly expressed in KIRC tissues, but they were prognostic protective factors for patients. This may be related to the specificity of the kidney organ. Different from other tumors, the immune infiltration of renal cancer is unique and may be related to the embryonic origin of renal development. During the SARS-CoV-2 epidemic, although ACE2, NRP1, and CTSL1 showed a protective effect, we cannot ignore the uniqueness of KIRC patients, who may be more susceptible to SARS-CoV-2 virus infection.</p><p>Second, we analyzed the effectiveness of three receptors, ACE2, NRP1, and CTSL1 as molecule targets against SARS-CoV-2 infection. According to the expression level, TCGA KIRC patients were divided into two categories with high or low expression based on each receptor's median expression level. Then, we detected the half-maximal inhibitory concentration response concentrations of the two types of patients to molecular inhibitors from the GDSC database. The results demonstrated that patients with high ACE2 expression were most sensitive to NSC.8787, erlotinib, and epothilone B (Figure S1). The chart lists the top five molecular inhibitors with the most significant differential responses. The patients with high expression of NRP1 were most sensitive to drugs such as Embelin, CHIR.99021, and VX.702. Patients with high CTSL1 expression showed more sensitivity to NSC.8787, MG.132, and sorafenib (Figure S1). From the intersection of the sensitive molecular inhibitors, eight molecular inhibitors with distinct differential reactivity were obtained, ranked according to <i>p</i> value including cyclopamine, epothilone B, FH535, gemcitabine, GSK.650394, JNK.9L, NSC.87877, and shikonin (Figure 1D). The COVID-19 Drug and Gene Set Library website also indicated that gemcitabine, GSK.650394, and shikonin had been experimentally tested as inhibitor drugs against the SARS-CoV-2 virus.<span><sup>4</sup></span> This result verified feasibility of ACE2, NRP1, and CTSL1 as SARS-CoV-2 inhibitory targets and reliability of our results. Cyclopamine, epothilone B, and FH535 have not yet undergone drug clinical trials, which is a valuable direction for subsequent research.</p><p>Finally, we analyzed the correlation of six infection receptors, ACE2, TMPRSS2, NRP1, AXL, FURIN, and CTSL1, with the signaling pathways in KIRC. The results indicated that ACE2 was significantly positively correlated with adipogenesis, bile acid metabolism, fatty acid metabolism, and PI3K–AKT–mTOR signaling pathways, while significantly negatively correlated with apical junction, hypoxia, KRAS, and TGF-β signaling pathways. NRP1 was positively related to the TGF-β signaling pathway, UV response, KRAS signaling pathway and mitotic spindle signaling pathway, and significantly negatively related to oxidative phosphorylation, cholesterol, and DNA repair. CTSL1 was positively correlated with glycolysis, mTORC1, and MYC signaling pathways, but negatively correlated with KRAS, myogenesis, and apical surface. Consistently, ACE2, NRP1, and CTSL1 were significantly positively correlated with the PI3K–AKT–mTOR and protein secretion signaling pathways (Figure 1E). Inhibiting the activation of these two signaling pathways may achieve the purpose of inhibiting SARS-CoV-2 infection.</p><p>Although ACE2, NRP1, and CTSL1 are favorable prognostic factors in patients with KIRC at the oncological level, the protection for KIRC patients should be strengthened during the SARS-CoV-2 epidemic, especially during the recent Omicron epidemic, which may be easily overlooked by oncologists.<span><sup>5</sup></span> In addition, targeting ACE2, NRP1, and CTSL1 were evaluated for effectiveness against SARS-CoV-2, and eight potential drugs were obtained. We also analyzed the enrichment of six host receptors in various KIRC signaling pathways.</p><p>In conclusion, although the receptors are protective factors for KIRC patients, their protection should also be strengthened because they may have a higher susceptibility to the SARS-CoV-2 virus. We should strike a balance between targeting these receptors and protecting renal cancer patients from the virus.</p><p><b>Aimin Jiang</b>: Conceptualization (equal). <b>Le Qu</b>: Formal analysis (equal); visualization (equal). <b>Bing Liu</b>: Formal analysis (equal); visualization (equal). <b>Anbang Wang</b>: Writing – original draft (equal). <b>Linhui Wang</b>: Conceptualization (equal). All authors have read and approved the article.</p><p>The authors declare no conflict of interest.</p><p>Not applicable.</p>","PeriodicalId":74135,"journal":{"name":"MedComm - Future medicine","volume":"2 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-01-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/mef2.31","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"MedComm - Future medicine","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/mef2.31","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
At the end of 2019, the new coronavirus began to spread around the world. World Health Organization named this virus SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2), which caused coronavirus disease (COVID-19). In most people without underlying medical conditions, symptoms of SARS-CoV-2 infection are often mild and nonlethal. However, patients with cancer have significantly higher rates of severe SARS-CoV-2 infection and disease-related mortality than normal individuals.1 Numerous studies have shown that progressive malignancy is an independent risk factor for severe SARS-CoV-2 infection and related death. The incidence of long-term sequelae of SARS-CoV-2 infection in cancer patients is estimated at 15%–30%.2 Although the use of vaccines has reduced the chance of severe SARS-CoV-2 infection incidence, large-scale trials often exclude cancer patients. It remains to be seen how effective and safe the vaccine is in cancer patients and how long it is durable. Multiorgan single-cell sequencing analysis confirmed that key receptors for SARS-CoV-2 infection in humans include ACE2 (angiotensin-converting enzyme 2), TMPRSS2 (transmembrane serine protease 2), NRP1 (neuropilin-1), AXL (AXL receptor tyrosine kinase), FURIN, and CTSL1 (cathepsin L1).3 SARS-CoV-2 infection may directly or indirectly lead to acute kidney injury, which may be related to the cytophilic effects of the virus and cytokine-induced systemic inflammatory responses. These receptors may play a key role in SARS-CoV-2 infection-induced acute kidney injury and even death. These key receptors provide crucial evidence for the development of antiviral drugs for SARS-CoV-2. However, further research on these receptors in cancer patients is warranted.
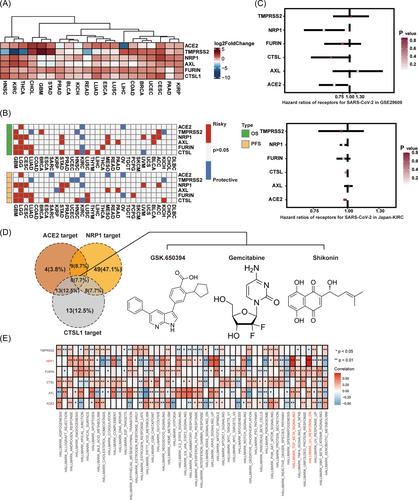
First, the expression profiling of prognosis prediction was investigated in multicancers. We found that except TMPRSS2, the remaining five receptors (ACE2, NRP1, AXL, FURIN, and CTSL1) were upregulated in various cancers, especially in kidney renal clear cell carcinoma (KIRC) (Figure 1A). The relationship between these receptors and the prognosis of cancer patients was analyzed. The results suggested that these four receptors, ACE2, NRP1, FURIN, and CTSL1, were prognostic risk factors in various cancers such as glioma, while in KIRC, they are protective factors for overall survival (Figure 1B). Similarly, ACE2, NRP1, and CTSL1 receptors were prognostic risk factors in gliomas and other tumors, and protective factors for disease progression-free survival in KIRC (Figure 1B). The protective induction of these three receptors on KIRC was also confirmed in the GSE29609 data set and the Japan-KIRC database (Figure 1C). The expression pattern of SARS-CoV-2 infection-related receptors in KIRC is different from other malignancies. ACE2, NRP1, and CTSL1 were highly expressed in KIRC tissues, but they were prognostic protective factors for patients. This may be related to the specificity of the kidney organ. Different from other tumors, the immune infiltration of renal cancer is unique and may be related to the embryonic origin of renal development. During the SARS-CoV-2 epidemic, although ACE2, NRP1, and CTSL1 showed a protective effect, we cannot ignore the uniqueness of KIRC patients, who may be more susceptible to SARS-CoV-2 virus infection.
Second, we analyzed the effectiveness of three receptors, ACE2, NRP1, and CTSL1 as molecule targets against SARS-CoV-2 infection. According to the expression level, TCGA KIRC patients were divided into two categories with high or low expression based on each receptor's median expression level. Then, we detected the half-maximal inhibitory concentration response concentrations of the two types of patients to molecular inhibitors from the GDSC database. The results demonstrated that patients with high ACE2 expression were most sensitive to NSC.8787, erlotinib, and epothilone B (Figure S1). The chart lists the top five molecular inhibitors with the most significant differential responses. The patients with high expression of NRP1 were most sensitive to drugs such as Embelin, CHIR.99021, and VX.702. Patients with high CTSL1 expression showed more sensitivity to NSC.8787, MG.132, and sorafenib (Figure S1). From the intersection of the sensitive molecular inhibitors, eight molecular inhibitors with distinct differential reactivity were obtained, ranked according to p value including cyclopamine, epothilone B, FH535, gemcitabine, GSK.650394, JNK.9L, NSC.87877, and shikonin (Figure 1D). The COVID-19 Drug and Gene Set Library website also indicated that gemcitabine, GSK.650394, and shikonin had been experimentally tested as inhibitor drugs against the SARS-CoV-2 virus.4 This result verified feasibility of ACE2, NRP1, and CTSL1 as SARS-CoV-2 inhibitory targets and reliability of our results. Cyclopamine, epothilone B, and FH535 have not yet undergone drug clinical trials, which is a valuable direction for subsequent research.
Finally, we analyzed the correlation of six infection receptors, ACE2, TMPRSS2, NRP1, AXL, FURIN, and CTSL1, with the signaling pathways in KIRC. The results indicated that ACE2 was significantly positively correlated with adipogenesis, bile acid metabolism, fatty acid metabolism, and PI3K–AKT–mTOR signaling pathways, while significantly negatively correlated with apical junction, hypoxia, KRAS, and TGF-β signaling pathways. NRP1 was positively related to the TGF-β signaling pathway, UV response, KRAS signaling pathway and mitotic spindle signaling pathway, and significantly negatively related to oxidative phosphorylation, cholesterol, and DNA repair. CTSL1 was positively correlated with glycolysis, mTORC1, and MYC signaling pathways, but negatively correlated with KRAS, myogenesis, and apical surface. Consistently, ACE2, NRP1, and CTSL1 were significantly positively correlated with the PI3K–AKT–mTOR and protein secretion signaling pathways (Figure 1E). Inhibiting the activation of these two signaling pathways may achieve the purpose of inhibiting SARS-CoV-2 infection.
Although ACE2, NRP1, and CTSL1 are favorable prognostic factors in patients with KIRC at the oncological level, the protection for KIRC patients should be strengthened during the SARS-CoV-2 epidemic, especially during the recent Omicron epidemic, which may be easily overlooked by oncologists.5 In addition, targeting ACE2, NRP1, and CTSL1 were evaluated for effectiveness against SARS-CoV-2, and eight potential drugs were obtained. We also analyzed the enrichment of six host receptors in various KIRC signaling pathways.
In conclusion, although the receptors are protective factors for KIRC patients, their protection should also be strengthened because they may have a higher susceptibility to the SARS-CoV-2 virus. We should strike a balance between targeting these receptors and protecting renal cancer patients from the virus.
Aimin Jiang: Conceptualization (equal). Le Qu: Formal analysis (equal); visualization (equal). Bing Liu: Formal analysis (equal); visualization (equal). Anbang Wang: Writing – original draft (equal). Linhui Wang: Conceptualization (equal). All authors have read and approved the article.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


