The combination of computed tomography-derived muscle mass and muscle density and relationship with clinicopathological characteristics and survival in patients undergoing potentially curative surgery for colorectal cancer
Abstract
Background
Sarcopenia has been defined as a loss of muscle mass and function. CT-derived muscle measurements, skeletal muscle index (SMI) and density (SMD), taken together may provide an objective measure of sarcopenia. The aim of the present study was to examine the relationship between CT-derived sarcopenia (low SMI and SMD), clinicopathological characteristics, systemic inflammation and survival in patients undergoing surgery for colorectal cancer.
Methods
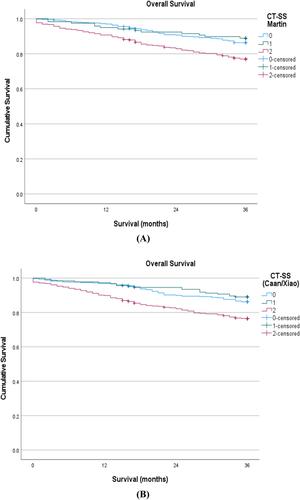
Consecutive patients who underwent resections for colorectal cancer (TNM I–III) at our institution, between April 2008 and 2018, were identified from a prospectively maintained database. CT-derived muscle mass (SMI) and density (SMD) measurements were combined to form the CT-Sarcopenia score (CT-SS). Thresholds for low SMI and SMD reported by Martin and co-workers and Caan/Xiao and co-workers were combined to form two iterations of the CT-SS. Patients were categorized as normal/high SMI (irrespective of SMD) = 0, low SMI and normal/high SMD = 1 and low SMI and low SMD = 2. The Pearson Chi square test was used to examine the associations between categorical variables and the Chi square test for linear trend was used for ordered variables with multiple categories. Survival data were analysed using univariate and multivariate Cox regression.
Results
One thousand and two patients met the study inclusion criteria. Fifty-five per cent (n = 554) of patients were male and 66% (n = 657) were aged 65 years or older. Twenty-four per cent (n = 240) of patients had TNM stage I disease, 40% (n = 404) stage II and 36% (n = 358) stage III. Eighteen per cent (n = 174) of patients were at risk of malnutrition. Forty-eight per cent (n = 479) of patients had an NLR ≥ 3 and 27% (n = 271) had an mGPS ≥ 1. Similar numbers of patients defined as CT-SS 0, 1 and 2 irrespective of thresholds applied (49%/12%/39% vs. 43%/19%/38%, respectively). Eight hundred and thirty four (n = 834) patients who underwent surgical resection for non-metastatic colorectal cancer with curative intent were alive at 3 years. On univariate analysis, both the CT-SS (Martin/Martin) and CT-SS (Caan/Xaio) were significantly associated with age (P < 0.001 and P < 0.001, respectively), ASA (P < 0.01 and P < 0.001, respectively), MUST (P < 0.001 and P < 0.005, respectively), mGPS (P < 0.001 and P < 0.001, respectively), NLR (P < 0.001 and P < 0.001, respectively), and overall survival (P < 0.001 and P < 0.001, respectively). CT-SS (Caan/Xaio) was significantly associated with TNM stage (P < 0.05), but not CT-SS (Martin/Martin, P = 0.221).
Conclusions
The objective CT-SS was significantly associated with older age, co-morbidity, nutritional risk, systemic inflammation and poorer survival, irrespective of thresholds used. However, the relationship between CT-SS and TNM stage was inconsistent and threshold dependent.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


