Paolo Boretto, Neal Hitesh Patel, Keval Patel, Mannat Rana, Andrea Saglietto, Manas Soni, Mahmood Ahmad, Jamie Sin Ying Ho, Ovidio De Filippo, Rui Andre Providencia, Jonathan James Hyett Bray, Fabrizio D'Ascenzo
{"title":"Prognosis prediction in cardiac amyloidosis by cardiac magnetic resonance imaging: a systematic review with meta-analysis.","authors":"Paolo Boretto, Neal Hitesh Patel, Keval Patel, Mannat Rana, Andrea Saglietto, Manas Soni, Mahmood Ahmad, Jamie Sin Ying Ho, Ovidio De Filippo, Rui Andre Providencia, Jonathan James Hyett Bray, Fabrizio D'Ascenzo","doi":"10.1093/ehjopen/oead092","DOIUrl":null,"url":null,"abstract":"<p><p>Cardiac involvement is the foremost determinant of the clinical progression of amyloidosis. The diagnostic role of cardiac magnetic resonance (CMR) imaging in cardiac amyloidosis has been established, but the prognostic role of various right and left CMR tissue characterization and functional parameters, including global longitudinal strain (GLS), late gadolinium enhancement (LGE), and parametric mapping, is yet to be delineated. We searched EMBASE, PubMed, and MEDLINE for studies analysing the prognostic use of CMR imaging in patients with light chain amyloidosis or transthyretin amyloidosis cardiac amyloidosis. The primary endpoint was all-cause mortality. A random effects model was used to calculate a pooled odds ratio using inverse-variance weighting. Nineteen studies with 2199 patients [66% males, median age 59.7 years, interquartile range (IQR) 58-67] were included. Median follow-up was 24 months (IQR 20-32), during which 40.8% of patients died. Both tissue characterization left heart parameters such as elevated extracellular volume [hazard ratio (HR) 3.95, 95% confidence interval (CI) 3.01-5.17], extension of left ventricular (LV) LGE (HR 2.69, 95% CI 2.07-3.49) elevated native T1 (HR 2.19, 95% CI 1.12-4.28), and functional parameters such as reduced LV GLS (HR 1.91, 95% CI 1.52-2.41) and reduced LV ejection fraction (EF; HR 1.20, 95% CI 1.17-1.23) were associated with increased all-cause mortality. Unlike the presence of right ventricular (RV) LGE (HR 3.40, 95% CI 0.51-22.54), parameters such as RV GLS (HR 2.08, 95% CI 1.6-2.69), RVEF (HR 1.13, 95% CI 1.05-1.22), and tricuspid annular systolic excursion (TAPSE) (HR 1.11, 95% CI 1.02-1.21) were also associated with mortality. In this large meta-analysis of patients with cardiac amyloidosis, CMR parameters assessing RV and LV function and tissue characterization were associated with an increased risk of mortality.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"3 5","pages":"oead092"},"PeriodicalIF":0.0000,"publicationDate":"2023-09-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3f/fc/oead092.PMC10575621.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oead092","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
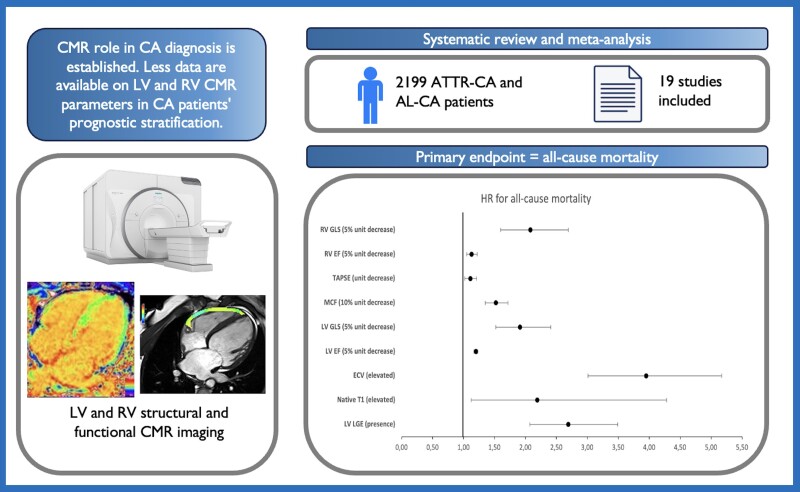
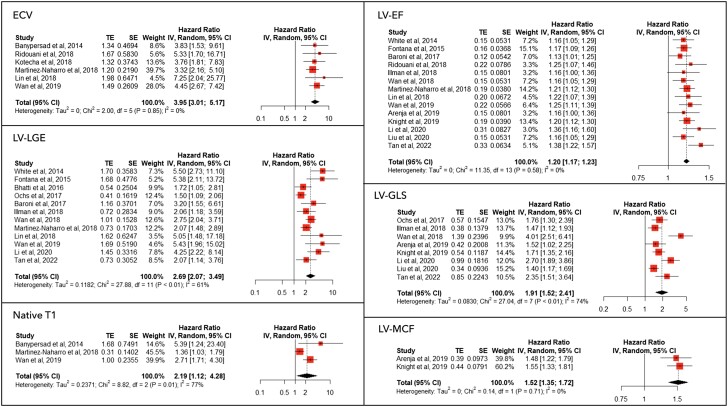
Cardiac involvement is the foremost determinant of the clinical progression of amyloidosis. The diagnostic role of cardiac magnetic resonance (CMR) imaging in cardiac amyloidosis has been established, but the prognostic role of various right and left CMR tissue characterization and functional parameters, including global longitudinal strain (GLS), late gadolinium enhancement (LGE), and parametric mapping, is yet to be delineated. We searched EMBASE, PubMed, and MEDLINE for studies analysing the prognostic use of CMR imaging in patients with light chain amyloidosis or transthyretin amyloidosis cardiac amyloidosis. The primary endpoint was all-cause mortality. A random effects model was used to calculate a pooled odds ratio using inverse-variance weighting. Nineteen studies with 2199 patients [66% males, median age 59.7 years, interquartile range (IQR) 58-67] were included. Median follow-up was 24 months (IQR 20-32), during which 40.8% of patients died. Both tissue characterization left heart parameters such as elevated extracellular volume [hazard ratio (HR) 3.95, 95% confidence interval (CI) 3.01-5.17], extension of left ventricular (LV) LGE (HR 2.69, 95% CI 2.07-3.49) elevated native T1 (HR 2.19, 95% CI 1.12-4.28), and functional parameters such as reduced LV GLS (HR 1.91, 95% CI 1.52-2.41) and reduced LV ejection fraction (EF; HR 1.20, 95% CI 1.17-1.23) were associated with increased all-cause mortality. Unlike the presence of right ventricular (RV) LGE (HR 3.40, 95% CI 0.51-22.54), parameters such as RV GLS (HR 2.08, 95% CI 1.6-2.69), RVEF (HR 1.13, 95% CI 1.05-1.22), and tricuspid annular systolic excursion (TAPSE) (HR 1.11, 95% CI 1.02-1.21) were also associated with mortality. In this large meta-analysis of patients with cardiac amyloidosis, CMR parameters assessing RV and LV function and tissue characterization were associated with an increased risk of mortality.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


