{"title":"Prevalence and prognostic value of atrial fibrillation in patients with cardiac sarcoidosis.","authors":"Yudai Fujimoto, Yuya Matsue, Daichi Maeda, Taishi Dotare, Tsutomu Sunayama, Takashi Iso, Yutaka Nakamura, Yu Suresvar Singh, Yuka Akama, Kenji Yoshioka, Takeshi Kitai, Yoshihisa Naruse, Tatsunori Taniguchi, Hidekazu Tanaka, Takahiro Okumura, Yuichi Baba, Takeru Nabeta, Tohru Minamino","doi":"10.1093/ehjopen/oead100","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>The prognostic value of the presence of atrial fibrillation (AF) in patients at the time of cardiac sarcoidosis (CS) diagnosis is unknown. This study aimed to investigate the association between AF at the time of CS diagnosis and patient prognosis.</p><p><strong>Methods and results: </strong>This study is a post-hoc analysis of Illustration of the Management and Prognosis of Japanese Patients with CS, a multicentre, retrospective observational study that evaluated the clinical characteristics and prognosis of patients with CS. The primary endpoint was the combined endpoint of all-cause death and hospitalization due to heart failure. After excluding patients with missing data about AF status, 445 patients (62 ± 11 years, 36% males) diagnosed with CS according to the Japanese current diagnostic guideline were analysed. Compared to patients without AF, patients with AF (<i>n</i> = 46, 10%) had higher levels of brain natriuretic peptide and a higher prevalence of heart failure hospitalizations. During a median follow-up period of 3.2 years (interquartile range, 1.7-5.8 years), 80 primary endpoints were observed. Kaplan-Meier curve analysis indicated that concomitant AF at the time of diagnosis was significantly associated with a high incidence of primary endpoints (log-rank <i>P</i> = 0.002). This association was retained after adjusting for known risk factors including log-transformed brain natriuretic peptide levels and left ventricular ejection fractions [hazard ratio, 1.96 (95% confidence interval, 1.05-3.65); <i>P</i> = 0.035].</p><p><strong>Conclusion: </strong>The presence of AF at the time of CS diagnosis is associated with higher incidence of all-cause death and heart failure hospitalization.</p>","PeriodicalId":93995,"journal":{"name":"European heart journal open","volume":"3 5","pages":"oead100"},"PeriodicalIF":0.0000,"publicationDate":"2023-09-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ab/ae/oead100.PMC10578462.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjopen/oead100","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
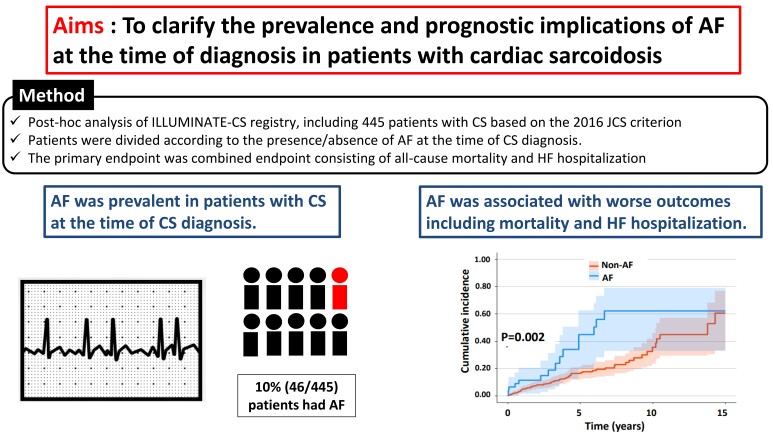
Aims: The prognostic value of the presence of atrial fibrillation (AF) in patients at the time of cardiac sarcoidosis (CS) diagnosis is unknown. This study aimed to investigate the association between AF at the time of CS diagnosis and patient prognosis.
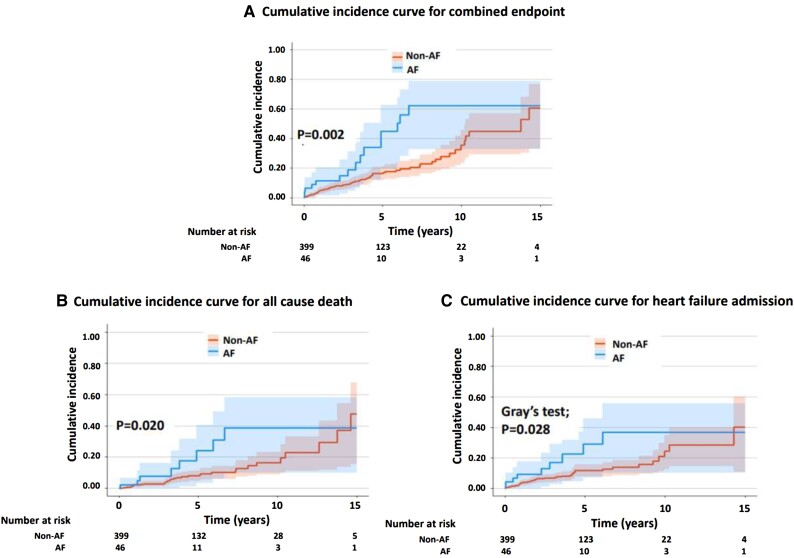
Methods and results: This study is a post-hoc analysis of Illustration of the Management and Prognosis of Japanese Patients with CS, a multicentre, retrospective observational study that evaluated the clinical characteristics and prognosis of patients with CS. The primary endpoint was the combined endpoint of all-cause death and hospitalization due to heart failure. After excluding patients with missing data about AF status, 445 patients (62 ± 11 years, 36% males) diagnosed with CS according to the Japanese current diagnostic guideline were analysed. Compared to patients without AF, patients with AF (n = 46, 10%) had higher levels of brain natriuretic peptide and a higher prevalence of heart failure hospitalizations. During a median follow-up period of 3.2 years (interquartile range, 1.7-5.8 years), 80 primary endpoints were observed. Kaplan-Meier curve analysis indicated that concomitant AF at the time of diagnosis was significantly associated with a high incidence of primary endpoints (log-rank P = 0.002). This association was retained after adjusting for known risk factors including log-transformed brain natriuretic peptide levels and left ventricular ejection fractions [hazard ratio, 1.96 (95% confidence interval, 1.05-3.65); P = 0.035].
Conclusion: The presence of AF at the time of CS diagnosis is associated with higher incidence of all-cause death and heart failure hospitalization.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


