{"title":"Customized cutoff limits for the sediMAX-2 automated analyzer reduce the number of urine culture tests.","authors":"Davide Ferrari, Mladen Trbos, Matteo Vidali, Massimo Locatelli","doi":"10.23750/abm.v94i5.14951","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Urinary tract infections are highly prevalent in nosocomial and community settings. Their diagnosis, although costly and time-consuming, is crucial to avoid inappropriate treatments and/or clinical complications. In this context, automated analyzers have been developed and commercialized to screen and rule out negative urine samples. Adjustments of the manufacturers' suggested cutoff values might lead to substantial diagnostic and economic advantages.</p><p><strong>Methods: </strong>We retrospectively analyzed 776 urine samples from different individuals. 546 samples (training group) were used to optimize develop new cutoffs values. The remaining 230 samples (validation group) were used to validate the optimized cutoffs. All samples were subjected to urine culture, 17% resulted positive. Escherichia coli and Enterococcus faecalis were the two most frequently identified bacteria, 95 and 9 samples, respectively.</p><p><strong>Results: </strong>Two different cutoffs levels were obtained. Cutoff-A (bacteria>110 and/or white blood cells> 15 cell/µL), showed the same sensitivity of the manufacturers' suggested cutoff, yet leads to a large reduction of the samples to be cultured. Cutoff-B (bacteria>50 and/or white blood cells>20 cell/µL), showed an almost 100% sensitivity by subjecting only ~70% of the samples to urine culture.</p><p><strong>Conclusion: </strong>Cutoff-A is a good compromise between sensitivity and specificity yet allowing economic advantages by reducing the number of urinary cultures. Cutoff-B relegates urinary tract infection misdiagnosis to a rare event without the need of culturing the entire batch of samples. We believe that clinical implementation of the proposed cutoffs will help other laboratories, using similar instrumentation, to reach their most convenient balance between sensitivity and economical needs.</p>","PeriodicalId":93849,"journal":{"name":"Acta bio-medica : Atenei Parmensis","volume":"94 5","pages":"e2023192"},"PeriodicalIF":0.0000,"publicationDate":"2023-10-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10644934/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta bio-medica : Atenei Parmensis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.23750/abm.v94i5.14951","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Urinary tract infections are highly prevalent in nosocomial and community settings. Their diagnosis, although costly and time-consuming, is crucial to avoid inappropriate treatments and/or clinical complications. In this context, automated analyzers have been developed and commercialized to screen and rule out negative urine samples. Adjustments of the manufacturers' suggested cutoff values might lead to substantial diagnostic and economic advantages.
Methods: We retrospectively analyzed 776 urine samples from different individuals. 546 samples (training group) were used to optimize develop new cutoffs values. The remaining 230 samples (validation group) were used to validate the optimized cutoffs. All samples were subjected to urine culture, 17% resulted positive. Escherichia coli and Enterococcus faecalis were the two most frequently identified bacteria, 95 and 9 samples, respectively.
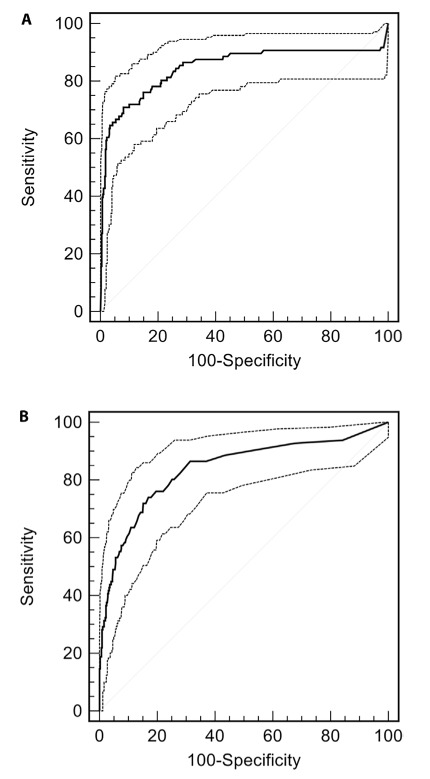
Results: Two different cutoffs levels were obtained. Cutoff-A (bacteria>110 and/or white blood cells> 15 cell/µL), showed the same sensitivity of the manufacturers' suggested cutoff, yet leads to a large reduction of the samples to be cultured. Cutoff-B (bacteria>50 and/or white blood cells>20 cell/µL), showed an almost 100% sensitivity by subjecting only ~70% of the samples to urine culture.
Conclusion: Cutoff-A is a good compromise between sensitivity and specificity yet allowing economic advantages by reducing the number of urinary cultures. Cutoff-B relegates urinary tract infection misdiagnosis to a rare event without the need of culturing the entire batch of samples. We believe that clinical implementation of the proposed cutoffs will help other laboratories, using similar instrumentation, to reach their most convenient balance between sensitivity and economical needs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


