{"title":"Rehabilitation after lumbar spine surgery in adults: a systematic review with meta-analysis.","authors":"Tiziana Manni, Nicola Ferri, Carla Vanti, Silvano Ferrari, Ilaria Cuoghi, Claudia Gaeta, Isabella Sgaravatti, Paolo Pillastrini","doi":"10.1186/s40945-023-00175-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The role of rehabilitation after surgery in patients with low back pain is well recognized. The aim of this systematic review is to summarize and update the existing evidence according to the type of clinical condition and rehabilitation approach.</p><p><strong>Methods: </strong>This systematic review included RCTs on the effectiveness of rehabilitation after surgery for lumbar disc herniation, spinal stenosis, and spondylolisthesis. We searched the literature for randomized controlled trials indexed in MEDLINE, Embase, CINHAL, CENTRAL, Scopus, PEDro, and Web of Science databases, up to April 15, 2023. We used Cochrane Risk of Bias 2.0 tool to assess each study. We conducted a quantitative synthesis when population, intervention, control, and outcome were sufficiently homogeneous; otherwise, we conducted a qualitative analysis.</p><p><strong>Results: </strong>Forty-five studies (3.036 subjects) were included and analyzed according to the population considered: lumbar stenosis (1 trial), spondylolisthesis (3 trials), and disc herniation (41 trials). Regarding lumbar stenosis, a supervised active exercise program appears to improve outcomes related to pain, disability, and quality of life both in the short- and mid-term (1 study, n = 60). Concerning spondylolisthesis, kinesiophobia is reduced in the home exercises group compared to usual care, at 3-months follow-up (3 studies, n = 98). For disk herniation, supervised exercises are better than non-supervised exercises to reduce pain (MD -1.14; 95% CIs -1.65, -0.62; 5 trials, n = 250) and disability (SMD -0.70; 95% CIs -1.14, -0.26; 4 trials, n = 175). Supervised exercises are better than advice in reducing pain (SMD -0.91; 95% CIs -1.61, -0.21; 5 trials, n = 341) and disability (SMD -0.80; 95% CIs -1.59, -0.01; 4 trials, n = 261), in the short-term. Supervised exercises are equal to no treatment in reducing pain and disability, at 3 and 6 months after intervention (2 trials, n = 166). These results are supported by a very low to low quality of evidence.</p><p><strong>Conclusions: </strong>Our research suggests that supervised exercise may be effective in improving patient's pain and disability after lumbar surgery, but RCTs regarding lumbar spinal stenosis and lumbar spondylolisthesis are still scarce, with significant heterogeneity of proposed interventions.</p>","PeriodicalId":72290,"journal":{"name":"Archives of physiotherapy","volume":"13 1","pages":"21"},"PeriodicalIF":2.9000,"publicationDate":"2023-10-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10578022/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archives of physiotherapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40945-023-00175-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"REHABILITATION","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The role of rehabilitation after surgery in patients with low back pain is well recognized. The aim of this systematic review is to summarize and update the existing evidence according to the type of clinical condition and rehabilitation approach.
Methods: This systematic review included RCTs on the effectiveness of rehabilitation after surgery for lumbar disc herniation, spinal stenosis, and spondylolisthesis. We searched the literature for randomized controlled trials indexed in MEDLINE, Embase, CINHAL, CENTRAL, Scopus, PEDro, and Web of Science databases, up to April 15, 2023. We used Cochrane Risk of Bias 2.0 tool to assess each study. We conducted a quantitative synthesis when population, intervention, control, and outcome were sufficiently homogeneous; otherwise, we conducted a qualitative analysis.
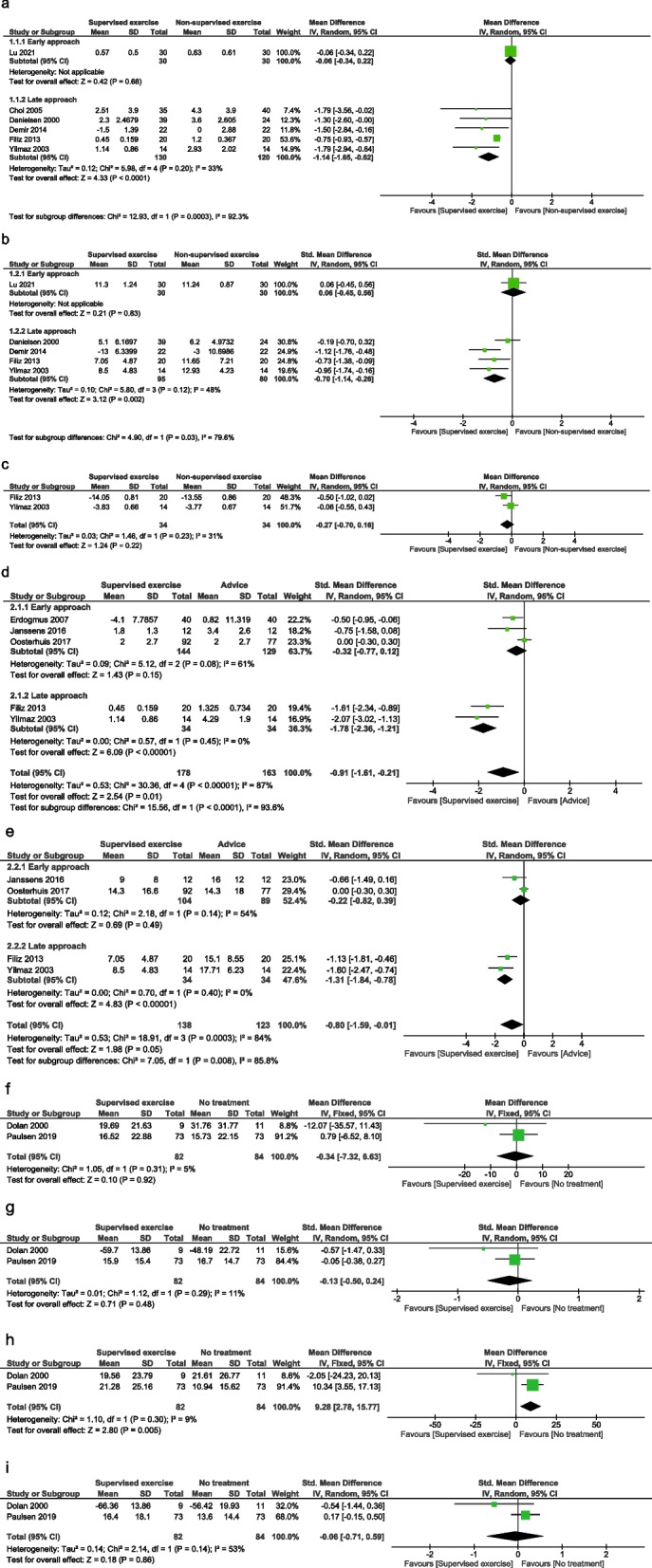
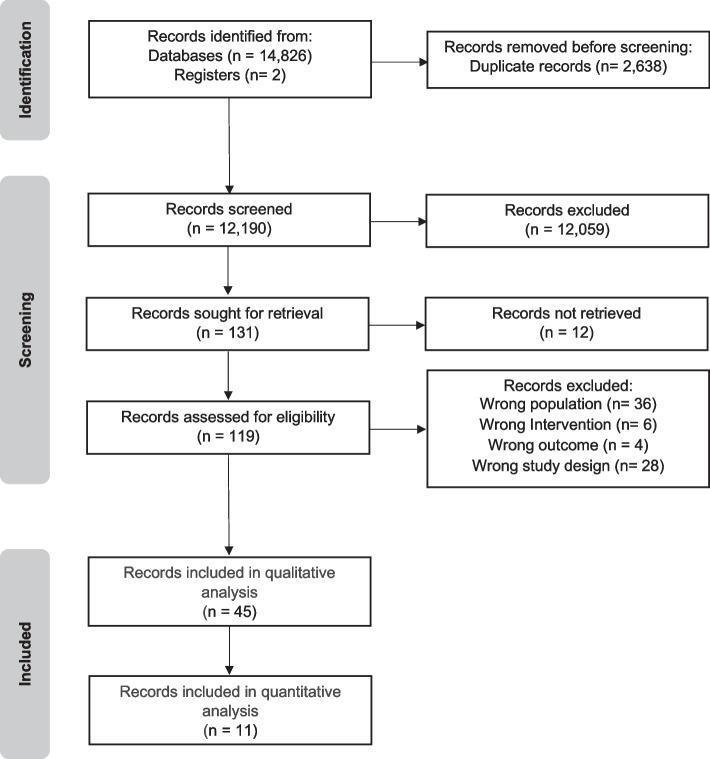
Results: Forty-five studies (3.036 subjects) were included and analyzed according to the population considered: lumbar stenosis (1 trial), spondylolisthesis (3 trials), and disc herniation (41 trials). Regarding lumbar stenosis, a supervised active exercise program appears to improve outcomes related to pain, disability, and quality of life both in the short- and mid-term (1 study, n = 60). Concerning spondylolisthesis, kinesiophobia is reduced in the home exercises group compared to usual care, at 3-months follow-up (3 studies, n = 98). For disk herniation, supervised exercises are better than non-supervised exercises to reduce pain (MD -1.14; 95% CIs -1.65, -0.62; 5 trials, n = 250) and disability (SMD -0.70; 95% CIs -1.14, -0.26; 4 trials, n = 175). Supervised exercises are better than advice in reducing pain (SMD -0.91; 95% CIs -1.61, -0.21; 5 trials, n = 341) and disability (SMD -0.80; 95% CIs -1.59, -0.01; 4 trials, n = 261), in the short-term. Supervised exercises are equal to no treatment in reducing pain and disability, at 3 and 6 months after intervention (2 trials, n = 166). These results are supported by a very low to low quality of evidence.
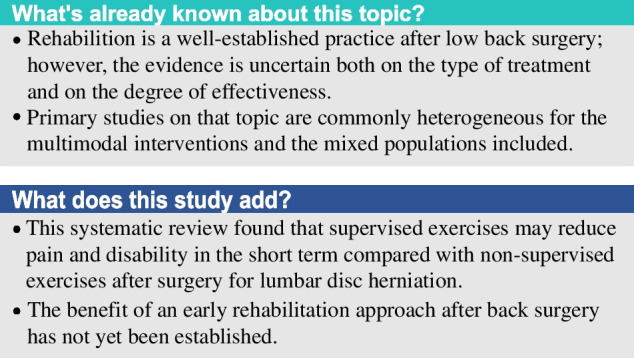
Conclusions: Our research suggests that supervised exercise may be effective in improving patient's pain and disability after lumbar surgery, but RCTs regarding lumbar spinal stenosis and lumbar spondylolisthesis are still scarce, with significant heterogeneity of proposed interventions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


