Julie B Gallois, Jessica A Zagory, Brian Barkemeyer, Michelle Knecht, Lauren Richard, Kathleen Vincent, David Sciacca, Crystal Maise-Dykes, Christy Mumphrey
{"title":"Handoff Tool Improves Transitions from the Operating Room to the Neonatal Intensive Care Unit.","authors":"Julie B Gallois, Jessica A Zagory, Brian Barkemeyer, Michelle Knecht, Lauren Richard, Kathleen Vincent, David Sciacca, Crystal Maise-Dykes, Christy Mumphrey","doi":"10.1097/pq9.0000000000000695","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Standardized handoffs reduce medical errors and prevent adverse events or near misses. This article describes a quality improvement initiative implementing a unique standardized handoff tool and process to transition from the operating room to the neonatal intensive care unit (NICU) at a level-four regional center with many inpatients requiring surgical intervention. Before this project, there was no standardized handoff tool or process for postsurgical transitions. The primary aim was to achieve 80% compliance with completing a structured postoperative OR to NICU handoff tool within 12 months of implementation.</p><p><strong>Methods: </strong>An interdisciplinary team developed and implemented a standardized NICU postoperative handoff tool and process that requires face-to-face communication, defines team members who should be present, and highlights communication with the family. In addition, the handoff tool compliance and process measures were monitored, evaluated, and audited.</p><p><strong>Results: </strong>Although not consistent, we achieved eighty percent compliance with the outcome measures using the handoff tool. We did not sustain 80% of appropriate providers present at handoff. In addition, insufficient data assess overall parental satisfaction with the surgical experience. Although improved, the process measure of immediate postoperative family updates did not reach the targeted goal. However, the balancing measure of staff experience and satisfaction did improve.</p><p><strong>Conclusion: </strong>Implementing a standardized handoff tool and process with an interdisciplinary and interdepartmental collaboration improves critical patient transitions from the operating room to the NICU.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"8 5","pages":"e695"},"PeriodicalIF":1.2000,"publicationDate":"2023-10-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10561795/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000695","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
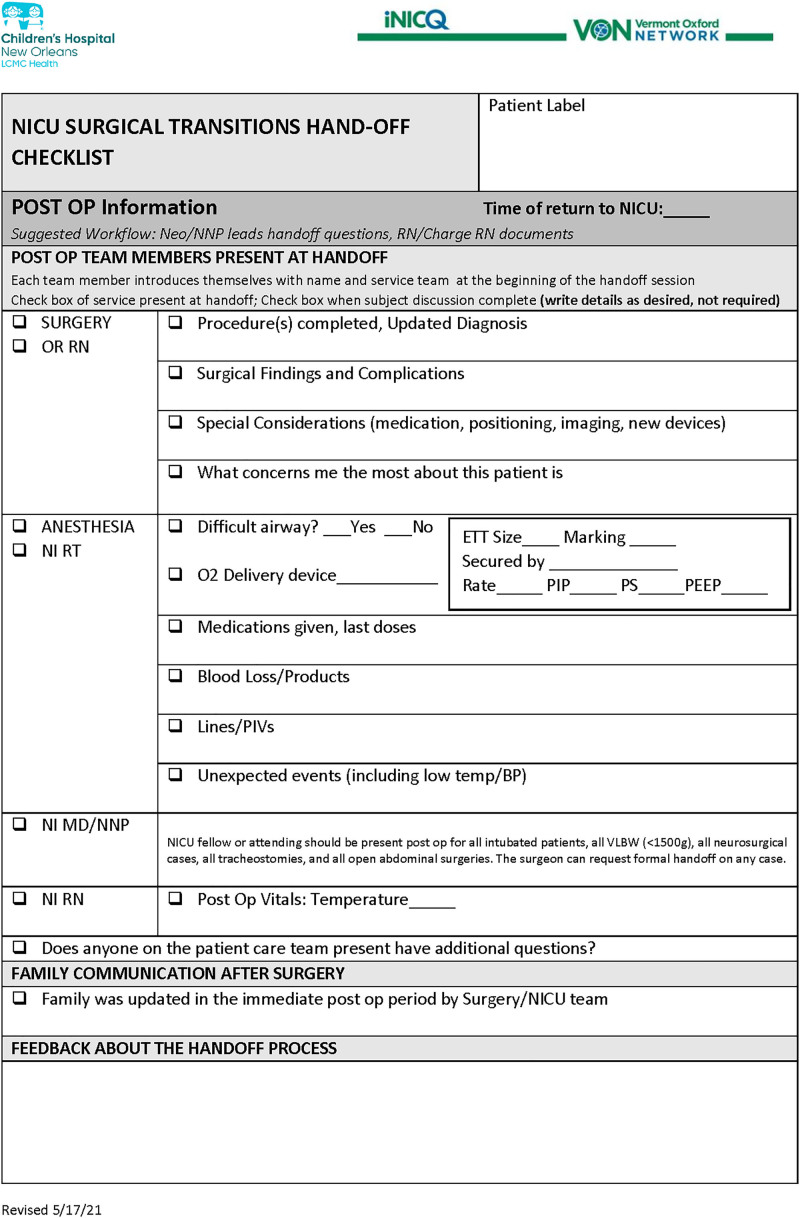
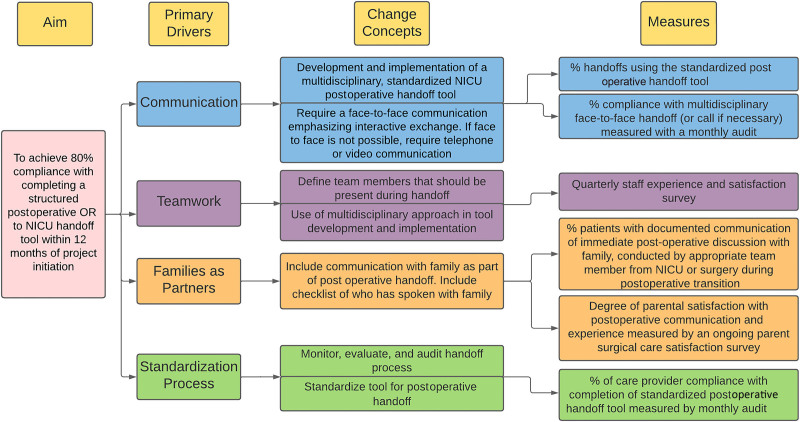
Introduction: Standardized handoffs reduce medical errors and prevent adverse events or near misses. This article describes a quality improvement initiative implementing a unique standardized handoff tool and process to transition from the operating room to the neonatal intensive care unit (NICU) at a level-four regional center with many inpatients requiring surgical intervention. Before this project, there was no standardized handoff tool or process for postsurgical transitions. The primary aim was to achieve 80% compliance with completing a structured postoperative OR to NICU handoff tool within 12 months of implementation.
Methods: An interdisciplinary team developed and implemented a standardized NICU postoperative handoff tool and process that requires face-to-face communication, defines team members who should be present, and highlights communication with the family. In addition, the handoff tool compliance and process measures were monitored, evaluated, and audited.
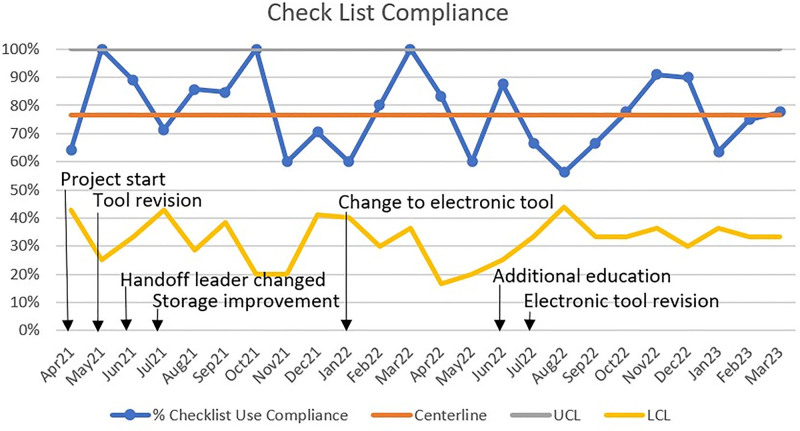
Results: Although not consistent, we achieved eighty percent compliance with the outcome measures using the handoff tool. We did not sustain 80% of appropriate providers present at handoff. In addition, insufficient data assess overall parental satisfaction with the surgical experience. Although improved, the process measure of immediate postoperative family updates did not reach the targeted goal. However, the balancing measure of staff experience and satisfaction did improve.
Conclusion: Implementing a standardized handoff tool and process with an interdisciplinary and interdepartmental collaboration improves critical patient transitions from the operating room to the NICU.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


